In an earlier study of Protestants and Jews in the UK we found that specific religious coping beliefs were related to emotional outcomes, in individuals under stress. In this study, we followed up 84 of the original 126 participants (33 Protestants, 51 Jews) to see whether religious coping beliefs related to outcomes nine months later. Outcomes studied were distress, positive affect, and intrusive thoughts. Religious activity and orientation, and religiously-based cognitions (at time 1), had detectable effects on outcomes nine months later at time 2. The most robust effects of the religious factors examined were on positive mood. The effects on long-term negative outcomes – distress and intrusive thoughts - were less marked than the effects on positive mood, although there were some indirect effects. The study suggested that the long-term effects of religious coping were more marked on positive than on negative affect. The study indicated some of the cognitive routes by which religion may affect the emotional impact of stress, and offers some support for the possibility that the stress-moderating effects of religious coping beliefs may be causal.
How does religion affect thinking, and in particular the interpretation of challenging and potentially distressing events? How might such religious thinking affect emotions?
Although religion has been suggested to have a generally positive relationship with well being, different features of religious activity, belief and coping have different relationships to well-being, distress and psychopathology (Pargament, 1997; Loewenthal, 2000; Koenig, McCullough and Larson, 2000). Recent work has started to disentangle some of the positive and negative relationships, and to explore the question of causality, with particular interest in positive and negative coping, and religious orientation, and their relations to positive and negative mental health outcomes (Smith, McCullough & Poll, 2003; Gene & Erin, 2005; Carpenter, Laney & Mezoulis, 2011).
This paper explores some of the cognitive means by which religion may affect long-term outcome in individuals under stress. We are particularly interested in the cognitive aspects of coping, in the ways in which these may be affected by religion, and in the effects these may have on long-term outcomes in terms of mood and distress. We investigate coping beliefs that might relate positively to better mental health outcomes. Pargament, Koenig and Perez (2000) found that benevolent religious reappraisals, and seeking religious support were among those religious coping methods that were associated with better adjustment, unlike for example spiritual discontent and belief in a punishing deity, which were associated with poorer outcomes. Our focus was on three specific aspects of benevolent religious beliefs: the belief that G-d is supporting, the belief that G-d is ultimately in control, and the belief that ultimately this (trouble) is all for the best. We have been interested in the extent to which these beliefs are said to be actively used by people experiencing serious difficulties, and in the extent to which reported use of these beliefs actually relates to mental health outcomes.
In a previous study, we studied adults who had undergone recent major stress (Loewenthal, MacLeod, Goldblatt, Lubitsch and Valentine, 2000). Overall religiosity (based on measures of religious activity and orientation) were, very reasonably, related to the likelihood of using religiously-based coping thoughts and beliefs. These in turn related to positive mood, which, in turn, went with lowered distress. There were also direct associations between religiosity, and seeing a relatively high proportion of good consequences, and positive mood.
We thought it noteworthy that the religiously-based coping beliefs that we assessed did not relate directly to distress, only to positive affect. This accords with the suggestion that positive and negative affect need to be separately assessed in outcome studies (Watson, Clark and Tellegen, 1988; Clark and Watson, 1988; MacLeod and Byrne, 1996).
So, if and when religion comforts, this is because it cheers, and this effect is partly mediated by cognitive means. But are these effects truly causal? Does good mood improve access to, or facilitate the generation of, positive cognitions, and poor mood, negative cognitions? Are moods driven by cognitions? Participants might, for example, have reported believing that they were being supported by G-d as a result of feeling cheerful, rather than spiritual support causing cheerful feelings? In a cross-sectional, or even in a retrospective study, there is usually this ambiguity in interpreting direction of effect.
The present study reports on the mood of participants nine months after first assessing religiosity and religious coping cognitions. This enabled us to discover whether there were any long-term effects, and allowed causal inferences about the direction of effect to be made with greater confidence.
The aims of this study were to follow up participants from an earlier study, to examine longer-term mood and distress outcomes, and to see whether these could be predicted by the measures of religiosity and religious coping studied nine months previously. We examined and tried to understand the similarities and differences between the best-fitting causal pathway model based on our first, retrospective and cross-sectional study, and the causal pathway model based on this second, prospective study.
METHOD
Participants
This study examines 84 adults participating in a follow-up study.
126 adults had completed the first phase of the study, and were followed-up nine months later. All participants were English-speaking and living in Southern England at the time of the study. Only participants who had suffered potentially depressogenic stress in the previous 12 months were admitted into the study. We followed strict contextual criteria for depressogenic stress, using Brown and Harris's (1978) definition of a provoking agent for depression. To sharpen the effects of religion, we included in the study only those with high (7-10) or low (0-3) self-ratings of religiousness. To study the effects of cultural-religious background, Protestants and Jews were recruited, but religious background (Protestant/Jewish) showed no noteworthy effects in the analyses. Although in other work differences in beliefs and behaviour relate to cultural-religious background, the measures we used showed no such effects, and we conclude that the Protestants and Jews in this study were essentially similar with respect to the coping beliefs studied, and their effects.
6-9 months after the first phase (T1) all participants were contacted for the second phase study (T2), and 2-3 months later, those failing to respond to the first follow-up request were re-contacted. Following these two requests, a total of 84 (67% of the 126 original participants) completed the second phase. Second phase participants were older, more likely to be married, and to be Jewish, than were the people who did not respond (table 1).
Table 1
Table 1 also shows that the groups of high and low-religious, and of Protestants and Jews, did not differ from each other with respect to gender, age or marital status, except that the low-religious were younger than the high-religious. Age was therefore partialled out in subsequent analyses.
Measures
For this follow-up study, table 2 summarises which measures were taken at time 1, and at time 2. The measures are described in detail below.
Table 2
Stress. This study included only those suffering from a level of stress at recruitment that was potentially depressogenic, using Brown and Harris's (1978) criteria for a provoking agent for depression. To assess stress, we used the contextual criteria developed by Brown and Harris, as follows: in the recruitment phase, all participants completed a life events and difficulties screening checklist consisting of the Life Events and Difficulties Schedule (LEDS; Brown and Harris, 1978) categories, followed-up with specific questions from the LEDS to establish the presence of a provoking agent for depression. The presence of a (potentially depressogenic) provoking agent was defined as follows: at least one self- or joint-focused event in the twelve months prior to interview, rated at least high-moderate on long-term contextual threat, and independent of any psychiatric illness; or at least one major difficulty, of at least high-moderate threat, ongoing for at least two years prior to interview, and still ongoing. Interviews and ratings were carried out by trained LEDS interviewers.
To assess the effects of intervening stress on the outcome measures at time 2, the LEDS checklist and interview was repeated at time 2, giving attention to whether the original stressor was unabated, resolved, or worse, and also attending to the occurrence of new stressors. On the basis of this, participants were rated for the presence of a provoking agent, and this factor (along with age) was partialled out in the causal pathway analysis.
Religiosity (religious activity and orientation). Participants self-assessed on three five-point scales indicating frequency of prayer, attendance at place of worship, and religious study (Loewenthal, MacLeod and Cinnirella, 2001) and completed Batson's (1976) three scales of religious orientation, which deal with the importance and extent of different types of religious activity, such as taking advice from clergy (extrinsic), applying religious teachings in daily life (intrinsic) and examining religious doubts (quest). All six measures proved to be significantly inter-correlated, and after standardising each component measure, were used to form an overall religiosity measure with a satisfactory Cronbach's alpha (0.75). Note that the extrinsic, intrinsic and quest scales are not usually inter-correlated among samples of religiously-active participants (Batson et al, 1993). In this study, however, a high proportion of low-religious participants was deliberately included. The high inter-correlation of the religious orientation scales indicates that they were functioning as a reflection of general religiosity, and they were used as such.
Cognitions.
All for the best. Two 10 cm. visual analogue scales were used, on which the participant indicated the extent to which they thought the (most severe) event or difficulty was all for the best, and the extent to which they now think the stressor is all for the best. These ratings were combined to give an overall measure, for which alpha = 0.89.
G-d control. Participants were asked to say why they thought the event or difficulty happened, and the number and proportion of G-d-control attributions was computed. Inter-rater agreement was 90% on a random selection of 10% of the ratings, made independently by two members of the research team.
Religious (Spiritual) Support Scale. The original term for this measure was the Spiritual Support scale (Maton, 1989), a term that became slightly misleading in the succeeding decade, with the rise of interest in spirituality as distinct from religiosity. This scale assesses the extent to which the person reports the use of religious constructs in coping, for example, "Religious faith has not been central to my coping". For this sample, Cronbach's alpha was 0.79.
Proportion of positive consequences. This measure used procedures developed and reported by MacLeod et al (1993), and MacLeod and Byrne (1996). Participants were asked to state all outcomes perceived to have resulted from, or been forestalled by the stressful event or difficulty. These responses were rated by the research team as "good", "bad" (or "neither" (7%)). A 10% sample of ratings was rated independently by two members of the research team, and inter-rater agreement was 95%. The proportion of good outcomes was calculated.
Intrusive unpleasant thoughts. Participants were asked to rate their thoughts about the stressor on three five-point Likert-type scales: for i) uncontrollability, ii) clarity and iii) unpleasantness of involuntary thoughts. The three items were significantly correlated (r ranged from 0.277 to 0.508, all significant at p<.001), and they formed a cohesive scale (alpha=0.79). This measure was repeated at T2
Of the cognitions measures, three are referred to as religiously-based cognitions: all for the best, G-d control, and religious/spiritual support.
Positive affect. the 10 positive-affect items from the PANAS (Positive and Negative Affect Scale; Watson, Clark and Tellegen, 1988) were used. Among the sample tested, alpha was 0.88 for the positive affect scale. This measure was repeated at T2.
Distress. The 10 negative-affect items from the PANAS (alpha=0.81 in this sample) were combined with the 7 depression and 7 anxiety items of the DSSI/sAD (Delusions-States-Symptoms Inventory/states of Anxiety and Depression), which is a 14-item Likert-type scale with seven depression and seven anxiety items, validated against psychiatrists' ratings, and showing good criterion validity (Bedford, Foulds and Sheffield, 1976). In both the PANAS and the DSSI/sAD participants were asked to rate the extent to which they had recently experienced the state/mood in question. The depression, anxiety and negative affect scores were significantly inter-correlated (r ranged from 0.513 to 0.765, all significant at p<.001), and the overall combined distress measure had an alpha of 0.72. These measures were repeated at T2.
RESULTS
Relations between religion, stress, cognitions and later intrusive thoughts, distress and positive mood.
Table 3 shows the partial correlations between the variables under study (with age partialled out).
TABLE 3
The noteworthy features of this table are first that stress was significantly related to the outcome measures, and thus in subsequent causal pathway analysis, it was necessary to partial out the effects of stress. Second, the religious coping cognitions (assessed at T1) generally related positively to positive mood. Relations with distress were weaker, and generally negative. Intrusive thoughts related to distress, and also to some of the religious cognition measures. Finally we noted that the positive outcomes measure (seeing a relatively high proportion of good compared to bad outcomes from the stressor) did not relate clearly to any of the other measures. The associations between religiosity, religious coping cognitions, and seeing positive outcomes on the one hand, and the measures assessed at T2 (positive mood, intrusive thoughts and distress) - were sufficiently like the associations with measures of the same factors at T1, for us to test the same model (Figure 1) that was found to fit the T1 data.
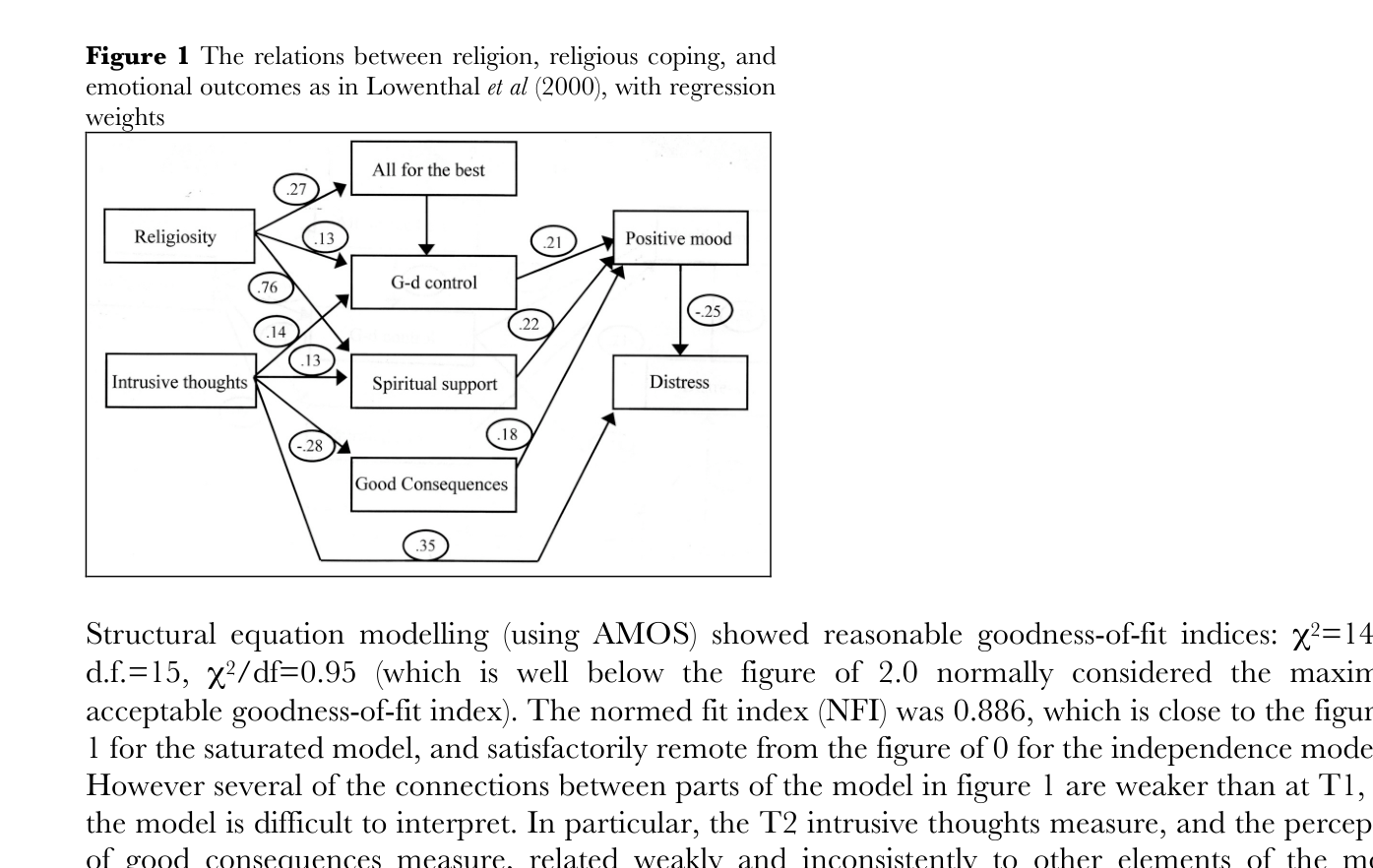
Structural modelling: Figure 1 shows the relationships in the causal pathway model (based on the data analysis at T1, as described in Loewenthal et al.)
FIGURE 1
Structural equation modelling (using AMOS) showed reasonable goodness-of-fit indices: X2=14.29, d.f.=15, X2/df=0.95 (which is well below the figure of 2.0 normally considered the maximum acceptable goodness-of-fit index). The normed fit index (NFI) was 0.886, which is close to the figure of 1 for the saturated model, and satisfactorily remote from the figure of 0 for the independence model.
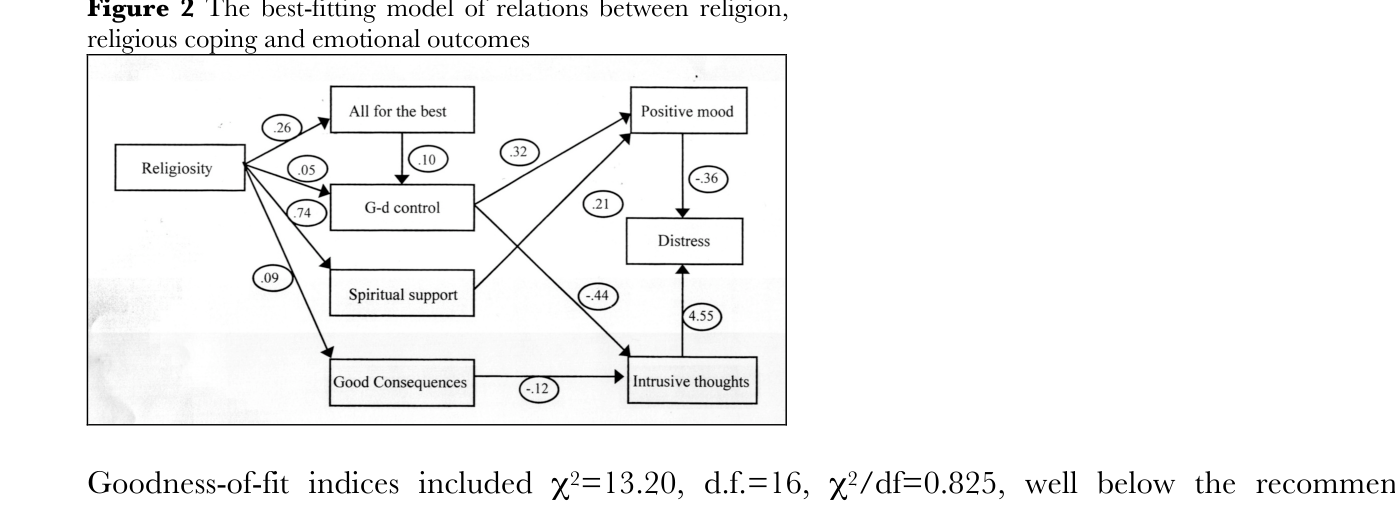
However several of the connections between parts of the model in figure 1 are weaker than at T1, and the model is difficult to interpret. In particular, the T2 intrusive thoughts measure, and the perception of good consequences measure, related weakly and inconsistently to other elements of the model (table 3). The model that best fitted the data is shown in Figure 2. The T2 intrusive thoughts measure has been treated as an outcome measure (as planned in the original research design), and the good consequences measure is shown not directly related to positive mood and distress outcomes, only to intrusive thoughts.
FIGURE 2
Goodness-of-fit indices included X2=13.20, d.f.=16, X2/df=0.825, well below the recommended maxinmum of 2.0; the normed fit index (NFI) was 0.872, which is close to the figure of 1 for the saturated model, and satisfactorily remote from the figure of 0 for the independence model. The main features of the model are that religiosity has direct effects on positive mood at follow-up, and the cognitons studied impacted directly or indirectly on positive mood at follow-up.
Other analyses
Further analyses were conducted to examine whether changes in affect from T1 to T2 related to the other factors measured. As might be expected, increased distress, intrusive thoughts and stress were associated, but none of the other variables – religion and cognitions measures – related to changes in affect in any noteworthy or consistent way, and these analyses will not be reported in detail.
DISCUSSION
This study has suggested that at least some of the stress-moderating effects of religion are cognitively-mediated, and can be predicted over reasonably long stretches of time - nine months in this study. This accords with other reports, such as Pargament, Koenig, Tarakeshwar & Hahn (2004), and Carpenter et al (2011).
To what extent were the relationships reported in the earlier retrospective and cross-sectional study supported by this prospective study?
Our major conclusion from our earlier cross-sectional study was that religiosity was associated with specific religious cognitions and beliefs, but these did not, as hypothesised, relate negatively to distress. In this study we are able to offer some evidence that the religious cognitions examined did relate to low levels of distress nine months later. The relations were indirect, and intrusive thoughts were clearly implicated in the relationship. The distress-lowering effects of religion and associated cognitions were somewhat stronger than in the earlier study. This is consistent with other suggestions that religion and/or religious belief may have a distress-lowering effect. Additionally, as in the first study, religious cognitions were associated were raised positive mood, and as in the retrospective study, positive mood was negatively associated with distress. This study is a prospective study, and the proposed direction of effect – that religious beliefs may lower distress and raise positive mood – is a viable suggestion about the direction of causality. Of course we cannot make the same assertion about the possibility that positive affect lowers distress, since these two measures were taken at the same point. Overall the first conclusion of this study is that there is broad support for the idea that religious cognitions can have generally beneficial effects on mood.
A second feature of our earlier findings is that the best-fit model was consistent with the suggestion that intrusive thoughts were stimulated by distress, which in turn stimulated any available religious beliefs. We thought this was a better interpretation of our data, than our original idea that intrusive thoughts might be reduced by religious beliefs. In this prospective study, the data best fit our original suggestion, namely that religious beliefs may lower intrusive thoughts, and hence distress. Thus distress-lowering effects of religious belief may operate via two pathways, first by raising positive affect (which may lower distress), and second, by lowering intrusive thoughts, which in turn relate to low levels of distress.
There are likely to be two independently-driven affect systems - positive and negative - and religion relates differently to each. The stronger relations were with positive affect - religious activity and orientation related nine months later to positive affect, and so too did related aspects of cognition: spiritual support, and (weakly) belief that all is controlled by G-d.
Thus there are at least two cognitive routes by which religion may affect outcomes in individuals under stress. One route involves perceived spiritual support, the belief that God is ultimately in control, and that ultimately all is for the best -the constellation of thoughts and feelings that are often subsumed under the term "faith". This route leads to positive mood, and our data suggest that positive mood is sustained by the cognitions involved. The second route involves intrusive thoughts. These – our current data suggest – are aroused by ongoing stress, and their presence strongly relates to distress. However our current data suggest that they may be alleviated by prior cognitions, particularly the belief that G-d is ultimately in control, and the perception of relatively good outcomes.
How did the religiously-related cognitions achieve their long-term effects? One possible pathway is that initially, stress arouses the available repertoire of consoling thoughts, including those based on religious activity and study. These are first applied in a fundamental cognitive appraisal of any stressful situation. It is not enough to "know", for example, that God is in control and that he will care for the individual; this "knowledge" has to applied to each specific stressful situation, and felt to be applicable. Once in place, this cognitive appraisal can be maintained with relative ease, and used to maintain positive mood, to reduce intrusive unpleasant thoughts, and (a less direct effect) to lower distress.
It has recently been shown (Rosmarin, Pirutinsky, Pargament & Krumrei, 2009) that Protestants, orthodox Jews and non-orthodox Jews differ in the extent to which beliefs about G-d’s benevolence are effective in reducing distress. Such beliefs are less effective for non-orthodox Jews. For orthodox Jews, religious activity was effective in addition to belief, in reducing distress. In this sample of UK Protestants and Jews we did not detect any Protestant-Jewish differences in the coping beliefs studied, or their effects. However, our analyses did include both Jews and Protestants who were not religiously identified, and out analyses confirmed that both these low-religious groups made little use of religious beliefs in coping with stress. Thus our findings generally confirm those of Rosmarin et al, though the lack of irreligious individuals of Protestant background in the Rosmarin et al study makes close comparison difficult.
There is a growing literature on religious coping among Jews (Loewenthal et al, 2000; Rosmarin, Pargament & Mahoney, 2009; Rosmarin et al 2009; Band, Dein & Loewenthal, 2011). This is a necessary addition to the large literature on coping among Christians, since we cannot assume that religious coping is similar in all religious-cultural groups. Further study of religious coping beliefs and practices in different religious groups is important.
It has been stressed that it is important to examine the effects of addressing spiritual and religious issues in psychotherapy and psychiatry (Pargament, 2007; Rosmarin et al, 2009; Cook, 2009. Our findings support this. We have suggested details of the ways in which spiritual practices lay the foundation for a repertoire of spiritual beliefs, which are called into play in coping with stress. It may be helpful to investigate the value of supporting this kind of cognitive appraisal in appropriate cases.
Acknowledgements
We are grateful to the Wellcome Trust for their generous support of this project (Grant No. 038946/Z/93/Z). We would also like to thank Helen Bicknell, Tessa Gorton, Tracey Francis and Paul Egbers for their assistance with interviewing and analysis. We thank many others who advised and helped, including Tirril Harris of the Medical Research Council Unit, Social Policy Department, Royal Holloway, for her tireless interest, and for patience in dealing with coding queries relating to the Life Events and Difficulties Schedule, Rosemary Westley for her practical support and advice on project management, and Chris Brewin, University College London, for his input into the design of the project. Last and most important, thanks to the participants who took time out during very difficult periods in their lives to answer our questions about how they coped.
References
Band, M., Dein, S. and Loewenthal, K.M. 2011 Religiosity, Coping and Suicidality within the Religious Zionist Community of Israel. A Thematic Qualitative Analysis. Mental Health, Religion and Culture 14(1):1-17.
Bedford, A., G.A.Foulds and B.F.Sheffield. 1976. A new personal disturbance scale. British Journal of Social and Clinical Psychology 15 (4): 387-394.
Bergin, A. 1991. Values and religious issues in psychotherapy and mental health. American Psychologist 46(4): 394-403.
Brown, G. and T.O.Harris. 1978. The Social Origins of Depression. London: Tavistock.
Carpenter, T.P., Laney, T. and Mezulis, A. 2011. Religious coping, stress and depressive symptoms among adolescents: A prospective study. Psychology of Religion and Spirituality 1(1)
Clark, L.A.. and D.Watson. 1988. Mood and the mundane: relations between daily life-events and self-reported mood. Journal of Personality and Social Psychology 54(2): 296-308.
Cook, C. 2009 Spirituality and Psychiatry. London: Royal College of Psychiatrists.
Gene, G.A. and Erin, B.V. 2005 Religious coping and psychological adjustment to stress.
Journal of Clinical Psychology 61(4): 461-480.
Loewenthal, K.M. 2000. The Psychology of Religion: A Short Introduction. Oxford: OneWorld.
Koenig, H.G., M.E. McCullough and D.E.Larson. 2000. A Handbook of Religion and Mental Health. New York: Oxford University Press.
Loewenthal, K.M., A.K.MacLeod and M.Cinnirella. 2001. Are women more religious than men? Gender differences in religious activity among different religious groups in the UK. Personality and Individual Differences 32: 133-139.
Loewenthal, K.M., A.MacLeod, V.Goldblatt, G.Lubitsch. and J.D.Valentine. 2000. Comfort and Joy? Religion, cognition and mood in individuals under stress. Cognition and Emotion 14(3): 355-374.
MacLeod, A.K. and A.Byrne. 1996. Anxiety, depression, and the anticipation of positive and negative experiences. Journal of Abnormal Psychology 105(2): 286-289.
Maton, K.I. 1989. The stress-buffering role of spiritual support: cross-sectional and prospective investigations. Journal for the Scientific Study of Religion 28(3): 310-323.
McIntosh, D. 1995. Religion-as-Schema, with implications for the relation between religion and coping. International Journal for the Psychology of Religion 5(1): 1-16.
Pargament, K.I. 1997. The Psychology of Religious Coping: Theory, Research and Practice. New York: Guilford.
Pargament, K.I., H.G.Koenig and L.M.Perez. 2000. A comprehensive measure of religious coping: Development and initial validation of the RCOPE. Journal of Clinical Psychology 56(4): 519-543.
Pargament, K.I., H.G.Koenig, N. Tarakeshwar and Hahn, J. 2004. Religious Coping Methods as Predictors of Psychological, Physical and Spiritual Outcomes among Medically Ill Elderly Patients: A Two-year Longitudinal Study. Journal of Health Psychology,
Rosmarin, D.H., Pargament, K.I. and Mahoney, A. 2009. The role of religiousness in anxiety, depression, and happiness in a Jewish community sample: A preliminary investigation. Mental Health, Religion and Culture 12(2): 97-114.
Rosmarin, D.H., Pirutinsky, S., Pargament, K.I. and Krumrei, E.J. 2009. Are religious beliefs relevant to mental health among Jews? Psychology of Religion and Spirituality 1(3): 180-190.
Smith, T.B., McCullough, M.E. and Poll, J. 2003. Religiousness and depression: Evidence for a main effect and the moderating influence of stressful life events. Psychological Bulletin 129(4): 614-636.
Watson, D., L.A.Clark and A.Tellegen. 1988. Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS scales. Journal of Personality and Social Psychology 54(6):1063-1070.
Table 1. Descriptive Statistics
|
Variable |
All Prot n=33 |
All Jew n=51 |
Lo Rel** n=39 |
Hi Rel** n=45 |
All N=84 |
All non-respondents n=45; any significant differences from respondents |
|
Gender |
F=17 M=16 |
F=35 M=16 |
F=21 M=18 |
F=31 M=14 |
F=52 M=32 |
F=26 M=16 |
|
Age* |
44.0 |
42.6 |
39.1 |
46.7 |
43.2 |
31.1 t=4.40*** |
|
Married Not now-married |
21 12 |
25 25 |
21 18 |
26 19 |
47 37 |
15 26 X2=21.87*** |
**High and low-religious refers to a preliminary self-rating on religiosity (0-3=low, 7-10=high) which was made at the point of recruitment into the study. In the main and follow-up study, religious activity and orientation was assessed as a continuous measure, described under "Measures".
*There was a significant main effect of religion on age, F1,81=5.10, p=.027.
Table 2: Measures taken at time 1 and at time 2
Time 1 Time 2 (nine months later) ____---__
Age
Stress (contextual stress) Ongoing stress
Religiosity (religious activity and orientation) Intrusive unpleasant thoughts about stressor
Extent of belief that all was for the best Positive affect
Extent of belief that G-d ultimately in control Distress (negative affect, anxiety, depression)
Spiritual support
Table 3: Inter-correlations between summary variables(with age partialled out)
|
|
Religiosity |
All-for-the-best |
G-d control |
Spiritual support |
Good consequences |
Positive affect |
Distress |
Intrusive thoughts |
|
Religiosity |
- |
- |
- |
- |
- |
- |
- |
- |
|
All-for-the-best |
.25* |
- |
- |
- |
- |
- |
- |
- |
|
G-d control |
.13 |
.23* |
- |
- |
- |
- |
- |
- |
|
Spiritual support |
.68*** |
.11 |
-.11 |
- |
- |
- |
- |
- |
|
Good consequences |
.09 |
.11 |
.05 |
.08 |
- |
- |
- |
- |
|
Positive affect |
.20~ |
-.08 |
.14 |
.22* |
-.08 |
- |
- |
- |
|
Distress |
.10 |
-.23* |
-.11 |
.17 |
-.23* |
.09 |
- |
- |
|
Intrusive thoughts |
.12 |
-.11 |
-.21~ |
.15 |
-.22* |
-.01 |
.52*** |
|
|
Stress |
.17 |
-.03 |
.07 |
.04 |
-.19~ |
.00 |
.52*** |
.40*** |