In recent decades, some agreement has been reached that there is a positive association between religion and mental health. This effect depends of course upon how both religion and mental health are defined, and the overall effect masks a number of specific effects that are negative as well as positive. However the overall effect is moderately robust (Bergin, 1991; Myers & Diener, 1995; Worthington, Kurusu, McCullough & Sandage, 1996).
Also in recent decades there has been a rapid growth of interest in the cognitive processes involved in reactions to stress, in distress, in psychological disorders and in therapy (Gotlib & Hammen, 1992; Williams, Watts, MacLeod & Mathews, 1988). In this study we adapted features of recent work on the cognitive aspects of emotion, in order to investigate some of the cognitive pathways that could account for aspects of any relationship between religion and mental health in individuals under stress.
Although it has been suggested that religiously-based cognitions may have important effects upon outcome in terms of wellbeing, health and lower distress (Pargament, Kennell, Hathaway, Grevengoed, Newman & Jones, 1988; Levin, 1994; McIntosh, 1995), systematic studies of specific religious cognitions in relation to outcomes are still in the very early stages of development and incorporation into the analysis of religion and coping.
Several studies suggest that religion affects causal analysis, description and interpretation of events. There is evidence of a theodicy effect, that religiosity involves or affects the perception of divine control over all or some events. Staples & Mauss (1987) examined the discourse of autobiographical accounts of committed (Protestant) Christians and found evidence of a "master attributional scheme", whereby all events in life are seen as fitting into an overall divine plan. Furnham & Brown (1992), Klonoff & Landrine (1994) and Loewenthal & Cornwall (1993) found that causal analyses of hypothetical distressing events including illnesses were affected by religiosity (including denomination) and by the nature of the event. In Loewenthal & Cornwall for instance, G-d was seen to be causal in the case of life-threatening illnesses and accidents, but not other events (relationship difficulties and financial problems). A widely reported corollary of religious belief and affiliation is the perception of purpose and meaning both in life and in specific events (Paloutzian, 1981; Staples & Mauss, 1987). Finally, there are several reports about religious support, namely the perception that G-d is enabling the sufferer to bear trouble and to cope. Loewenthal (1992) noted that Jewish participants reported that such support was sought and perceived to be helpful, and unpublished data from a study by Prudo, Harris & Brown (1984) suggested a similar effect for Protestant women. Maton (1989) quantified the extent of perceived spiritual (religious) support and showed that it had a stress-buffering effect under some conditions, among the Protestants studied.
Work on the emotions and the emotional disorders has indicated links between these disorders and causal analysis, description and interpretation of events (Clark & Teasdale, 1982; Williams & Hargreaves, 1994). One striking claim is that depression may be linked to an attributional style, persistently ascribing events (especially failure) to internal, stable and global factors. Some work has suggested the possibility of such attributional bias in depression (Gotlib & Hammen, 1992; Williams & Hargreaves, 1994; Williams, Watts, MacLeod & Mathews, 1988), and in a related vein, Janoff-Bulman (1979) has implicated characterological self-blame as a feature of depression.
Another claim is that distressed mood can affect differentially the retrieval of positively and negatively toned memories and ideas, particularly in the direction that depressed people are less able to generate positively toned thoughts and memories. This leads to a gloomy view of personal history, and a pessimistic view of ones personal future . This in turn may have a deleterious effect on mood, by propelling the sufferer into a spiral of brooding and further dejection (MacLeod & Byrne, 1996; MacLeod, Rose & Williams, 1993).
To risk over-simplification for the sake of making a clear contrast, we might summarise these two traditions of investigation as follows. The religious individual sees G-d as an ultimate cause, and even if things are bad there is a concealed ultimate good, and sees grounds for basic optimism. The depressed individual blames the self, especially if things are bad, and sees nothing to hope for. These two lines of causal analysis lead on the one hand to trust, and on the other to self-blame and despair. In this simplified outline, then, it is possible to suggest that religious ideas might lead to better mental health outcomes, especially in adverse circumstances.
This outline is consistent with some of the existing evidence, but it is quite speculative. It forms a background for this present attempt to assess specific cognitions among people who had recently undergone severe stress, to examine whether these cognitions were related to religiosity and to religious background, and to examine their relations to mental health outcomes. We followed the general position of Lazarus & Folkman (1984) and Pennebaker (1985), who suggest that cognitive reappraisal is important in combating morbid rumination, and suggest that religion may provide a repertoire of ideas helpful in such cognitive reappraisal. In this study we were not focusing on religious ideas which might be associated with poor outcomes, such as “G-d is punishing me”, or “G-d is not listening to my prayers” (Batson, Schoenrade & Ventis, 1993; Pargament & Brant, 1998; Wallston, Malcarne, Flores, Hansdottir, Smith, Stein, Weisman & Clements, in press).
We examined three sets of beliefs – religious coping cognitions - that have previously been linked with religion: first, that everything is for the best (Paloutzian, 1981; Staples & Mauss, 1987); second, that G-d is in control; third, that G-d is supporting the individual enabling one to bear pain and suffering (Maton, 1989). We examined three aspects of cognition that have previously been linked to depression: first, the ability to generate or retrieve positively- and negatively-toned specific ideas about the bad situation; second, the attributional analysis of events in terms of internal, stable and global factors; third, the inability to generate any explanation for the situation (Brewin, 1992). Finally, in line with recent research indicating that positive affect and wellbeing are important variables in mental health (Fava, Rafanelli, Cazzaro, Conti, & Grandi, 1998; Watson, Clark, & Tellegen, 1988) we examined positive affect separately from distress.
Most work on the stress-moderating effects of religion has looked at Christians and those from a Christian background, usually Protestant. In this study we sought to extend examination of effects of religion to include those from a different religious tradition, Judaism. There have been claims that psychiatric epidemiology may differ in Jewish compared to Christian populations (e.g. Levav, Kohn, Golding & Weissman, 1997; Sanua, 1989), as may relevant social factors (Loewenthal, Goldblatt, Gorton, Lubitsh, Bicknell, Fellowes & Sowden, 1995, 1997a, 1997b). Some of these may be associated with differences in cognitive aspects of coping.
In view of the wide range of definition and measurement of religiosity, we chose to operationalize religiosity by assessing behaviours, attitudes and values common to the institutions of both the religious traditions studied: prayer, attendance at public worship, and religious study, together with three measures of orientation to religion, extrinsic, intrinsic and quest. Measures of orientation to religion were developed by Allport & Ross (1967) and Batson (1975) to account for the complex associations between religion and prejudice, and other aspects of personality, attitudes and wellbeing (Batson et al 1993).
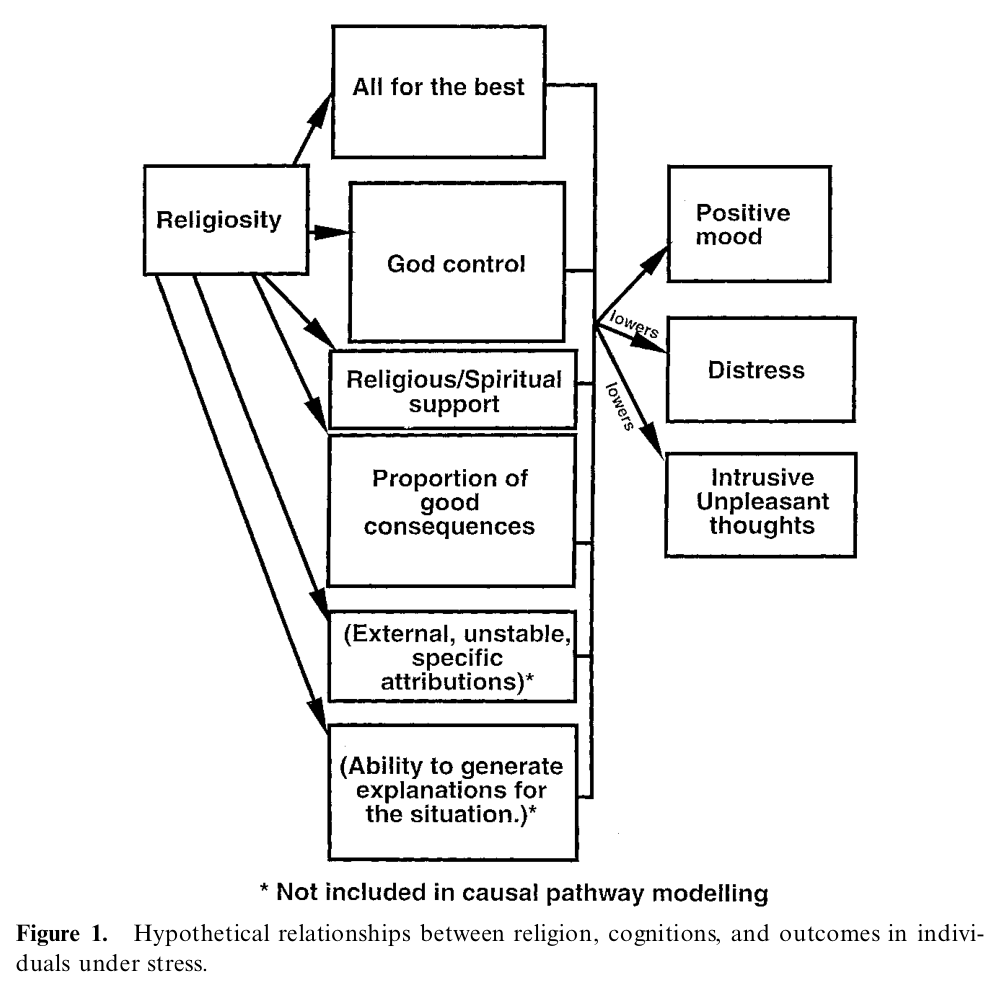
This study therefore looked to see whether cognitive aspects of coping were related to religiosity and to religious background, and whether these cognitive aspects of coping were related to wellbeing and distress. There were three main hypotheses. The first hypothesis was that religiosity would be associated with certain coping cognitions (an increased belief that all is for the best, that G-d is in control, and is providing support) and that such cognitions would in turn be associated with lowered distress. Second, we predicted that the generation of positive - as opposed to negative - consequences of the stressful event, and providing external, unstable and specific attributions for its occurrence, and being able to provide any explanations at all, would be related to lowered distress. Thirdly, we predicted that these consequence and attributional measures would also mediate the relationship between religiosity and distress. An exploratory aspect of the work was to examine the moderating role that positive affect might have on distress and how that role relates to religiosity and the cognition variables measured. No hypotheses could be advanced about whether cognition and outcome would differ by religious tradition (Protestant/Jewish). As the hypotheses concern the causal inter-relationship of a number of variables a path diagram best illustrates them. Figure 1 summarises the proposed hypothetical relationships between religion, cognition and outcomes.
INSERT FIGURE 1 ABOUT HERE
Method
Participants
One hundred twenty six participants were targeted at the recruitment stage: sixty eight Protestants and fifty eight Jews. All were suffering high levels of stress as defined below. Three Protestant and three Jewish interviewers acted as centres of "snowballs". Recruiting was via the Royal Holloway subject panel, synagogue and church groups, and personal contacts. Interviewers were required to identify participants with the target characteristics for religious background (Protestant, Jewish), and likely high levels of stress. Only about one person in three was expected to be suffering sufficiently severe stress to qualify for inclusion (Brown & Harris, 1978), and interviewers were asked to use their knowledge of potential participants in selecting those to be approached. Participants were also targeted for age, gender, marital status and general religiosity as recruitment proceeded, so as to ensure comparability of Protestants and Jews on these features. Protestants were defined as those with current affiliation with a Protestant church (mostly United Reformed Church, Church of England, and Baptist), or in the case of the unaffiliated, both parents defined as Protestant. Jews were defined as those affiliated with an orthodox synagogue (United Synagogue, Union of Orthodox Hebrew Congregation, Sefardic or Federation, accounting for about 80% of affiliated Jews in the UK: Shmool & Cohen, 1990), or in the case of the unaffiliated, both parents defined as Jews. All participants were English-speaking and living in Southern England at the time of the study.
The mean age of all participants was 39.1 years, 49% were now-married and 62% were women. There were no differences between Protestants and Jews with respect to these variables. We targeted a high proportion of participants who self-rated as low religious, and to check for possible unwanted confounded effects of religiosity we compared the religiously affiliated (n=69) with the unaffiliated (n=57). There were no significant differences in proportions of women and of the now-married. The affiliated were older than the unaffiliated (mean 43.4 years versus 35.4 years, t(121) = 2.54, p=.012), but when we ran our correlational analyses (Table 2), partialling out age had no appreciable effects.
Materials
Stress. This study included only those suffering from a level of stress that was potentially depressogenic, using Brown & Harris's (1978) criteria for a provoking agent for depression. To assess stress, we used the contextual criteria developed by Brown & Harris, as follows: in the recruitment phase, all participants completed a life events and difficulties screening checklist consisting of the Life Events and Difficulties Schedule (LEDS; Brown & Harris, 1978) categories, followed-up with specific questions from the LEDS to establish the presence of a provoking agent for depression. The presence of a (potentially depressogenic) provoking agent was defined as follows: at least one self or joint-focused event in the twelve months prior to interview, rated at least high-moderate on long-term contextual threat, and independent of any psychiatric illness; or at least one major difficulty, of at least high-moderate threat, ongoing for at least two years prior to interview, and still ongoing. Interviews and ratings were carried out by trained LEDS interviewers, in liaison with Tirril Harris and the Medical Research Council rating team in the Social Policy Department, Royal Holloway College, London University.
To check that the groups were comparable on types of stress, stress events and difficulties were classified as health-related, finance/employment-related, and relationships-related; the two groups were comparable on type of stress (Table 1). Thus any Protestant-Jewish differences could not be accounted by differing types of stress.
INSERT TABLE 1 ABOUT HERE
Religiosity (religious activity and orientation). Participants self-assessed on a range of five-point scales indicating frequency of prayer, attendance at place of worship, and religious study, and Batson's (1976) three scales of religious orientation, which deal with the importance and extent of different types of religious activity, such as taking advice from clergy (extrinsic), applying religious teachings in daily life (intrinsic) and examining religious doubts (quest). All six measures proved to be significantly inter-correlated, and after standardising each component measure, were used to form an overall religiosity measure with a satisfactory Cronbach's alpha (0.75). Note that the extrinsic, intrinsic and quest scales are not usually inter-correlated among samples of religiously-active participants (Batson et al, 1993). In this study, however, a high proportion of low-religious participants was deliberately included. The high inter-correlation of the religious orientation scales indicates that they were functioning as a reflection of general religiosity, and they were used as such.
Cognitions. (1) All for the best. Two 10 cm. visual analogue scales were used, on which the participant indicated the extent to which they thought the (most severe) event or difficulty was all for the best, and the extent to which they now think the stressor is all for the best. These ratings were combined to give an overall measure, for which alpha = 0.89. (2) G-d control and other causal attributions. Participants were asked to say why they thought the event or difficulty happened. The material was coded using Stratton, Heard, Hanks, Munton, Brewin & Davidson's (1986) causal attributional coding scheme, as follows: causal attributions in each statement were classified as internal vs. external, global vs. specific, stable vs. unstable, personal vs. universal, and uncontrollable vs. controllable, using Stratton et al's guidelines, with an additional category for causal attributions to G-d. Inter-rater agreement was 90% on a randomly-selected sample of 10% of the ratings, made independently by two members of the research team. As well as computing the number and proportion of G-d-control and other types of causal attribution, the presence/absence of internal + stable + global attributions was also computed for each subject. (3) Religious (Spiritual) Support Scale. This was originally termed the Spiritual Support scale(Maton, 1989). In spite of Maton’s original title for this scale, we were not concerned with assessing spirituality as a separate construct from religiosity (Zinnbauer, Pargament, Cole et al, 1997). Maton's three-item scale assesses the extent to which the person reports the use of religious constructs in coping, for example, "Religious faith has not been central to my coping", and was used as a measure of this (and not of spirituality). For this sample, Cronbach's alpha was 0.79. (4) Proportion of positive consequences. This measure used procedures developed and reported by MacLeod et al (1993), and MacLeod & Byrne (1996). Participants were asked to state all outcomes perceived to have resulted from, or been forestalled by the stressful event or difficulty, and were given a time limit of one minute to generate as many outcomes as they could. This elicited specific good and bad consequences of events, rather than (as in 1) examining global feelings that all is for the best. Participants were asked to describe both current and anticipated consequences of the stressor. These responses were later rated by the research team as "good", "bad" (or "neither" (7%); A 10% sample of ratings was rated independently by two members of the research team, and inter-rater agreement was 95%. The proportion of good outcomes was calculated. (5) Intrusive unpleasant thoughts. Participants were asked to rate their thoughts about the stressor on seven 5-point Likert-type scales: for i) frequency, ii) uncontrollability, iii) clarity and iv) unpleasantness of involuntary thoughts, and the v) frequency, vi) comfort and vii) helpfulness of deliberate thoughts about the stressor. Item analysis indicated that the three items assessing uncontrollability, clarity and unpleasantness were significantly correlated (r ranged from 0.277 to 0.508, all significant at p<.001), and formed a cohesive scale (alpha=0.79). This three-item scale was used as a measure of intrusive, unpleasant thoughts. The other thoughts ratings proved uncohesive and were not used further.
Of the cognitions measures, three will be referred to as religiously-based cognitions: all for the best, G-d control (from the causal attributions measures), and religious/spiritual support.
Positive affect. the 10 positive-affect items from the PANAS (Positive and Negative Affect Scale; Watson, Clark & Tellegen, 1988) were used. Among the sample tested, alpha was 0.88 for the positive affect scale.
Distress. The 10 negative-affect items from the PANAS (alpha=0.81 in this sample) were combined with the 7 depression and 7 anxiety items of the DSSI/sAD (Delusions-States-Symptoms Inventory/states of Anxiety and Depression), which is a 14-item Likert-type scale with seven depression and seven anxiety items, validated against psychiatrists' ratings, and showing good criterion validity (Bedford, Foulds & Sheffield, 1976). In both the PANAS and the DSSI/sAD participants were asked to rate the extent to which they had recently experienced the state/mood in question. The depression, anxiety and negative affect scores were significantly inter-correlated (r ranged from 0.513 to 0.765, all significant at p<.001), and the overall combined distress measure had an alpha of 0.72.
Procedure
Screening. Potential participants were identified, approached individually by one of the researchers, and asked if they would participate in a study of stress and religion. They were asked to complete a questionnaire with demographic information, a 0-10 self-rating of religiosity, a LEDS checklist covering the previous 12 months, and a written description of events and difficulties. Potential participants with moderate self-ratings on religiosity (4-6) were excluded from further study, to avoid the risk of overwhelming the study with large numbers of religious moderates who might obscure effects of religiosity and also to exclude those who were undecided. As recruitment proceeded we targeted participants with high or low self-ratings on religiosity as appropriate, to achieve comparability between Protestants and Jews. Sufficient questions from the Life Events and Difficulties Schedule were asked to establish whether or not a recent severe event or current major difficulty was likely, and those clearly without such major stress were excluded from further study. As recruitment proceeded further, we did not approach those who would unbalance the groups with regard to age, gender and marital status. None of those approached declined to participate. Of those who completed the screening questionnaire, two were excluded from further study since their level of stress was judged by the research team to be insufficiently high, and one further person was excluded since they did not meet the criteria for religious background.
Main phase. Participants who met criteria from the screening phase and who were willing to take part in the full study were asked to complete all measures in the same testing session. If participants reported more than one stressor they were asked to focus on the most severe or difficult. Measures were completed in the following order by all participants: Religiosity (religious activity and orientation), distress and positive affect, intrusive unpleasant thoughts, and whether the stressor was seen as all for the best. Participants then wrote a short paragraph on why they thought the event/difficulty had happened (for causal attributional analysis), and then described all consequences of the stressor, both good, bad and neutral, both current and anticipated. Finally, participants were thanked for their participation, and were offered the opportunity for questions about the study, and to leave an address (to be stored independently of data to preserve anonymity) for results of the study.
Results
Data reduction
On the basis of preliminary some measures were eliminated or collapsed to clarify further analysis. First, there were no significant Protestant-Jewish differences on the religiosity and cognition variables, and on the positive mood and distress measures. These non-significant effects of religious tradition have not been presented in more detail. Second, all except that G-d control measure of the causal attributional measures were eliminated: External, stable, specific attributions, and failing to offer explanations, were unrelated both to religiosity and to the outcome measures. These attributional measures are not reported further in any detail. Third, the three Batson scales of religious orientation failed to show associations with other variables and have not been reported separately. The religious orientation scales were however standardised and combined with standardised scores from the religious activity measures. This yielded a more sensitive measure of overall religiosity than the initial self-rated religiosity. For the overall religiosity measure, Cronbach’s alpha was 0.75. Finally, the overall distress measure was derived from the measures of negative affect, and of depression and anxiety, as described.
Relationships between the main variables
Table 2 shows the Pearson correlations between eight measures: religosity (religious activity and orientation), three religious coping variables (all for the best, G-d control and religious support), the proportion of good consequences, and three outcome measures (positive mood, distress, and intrusive unpleasant thoughts.
INSERT TABLE 2 ABOUT HERE
Religiosity was associated with the three religious coping cognitions, albeit weakly with G-d control, as hypothesised, but these cognitions were not in turn associated with lowered distress. The generation of positive compared to negative consequences was associated with lowered distress, as hypothesised. However this was a weak association. The consequences measure was related to religiosity, as hypothesised, although weakly. Religiosity was associated with positive mood, as were two of the religious cognitions measures, and the consequences measure.
Structural modelling of the predicted relationships
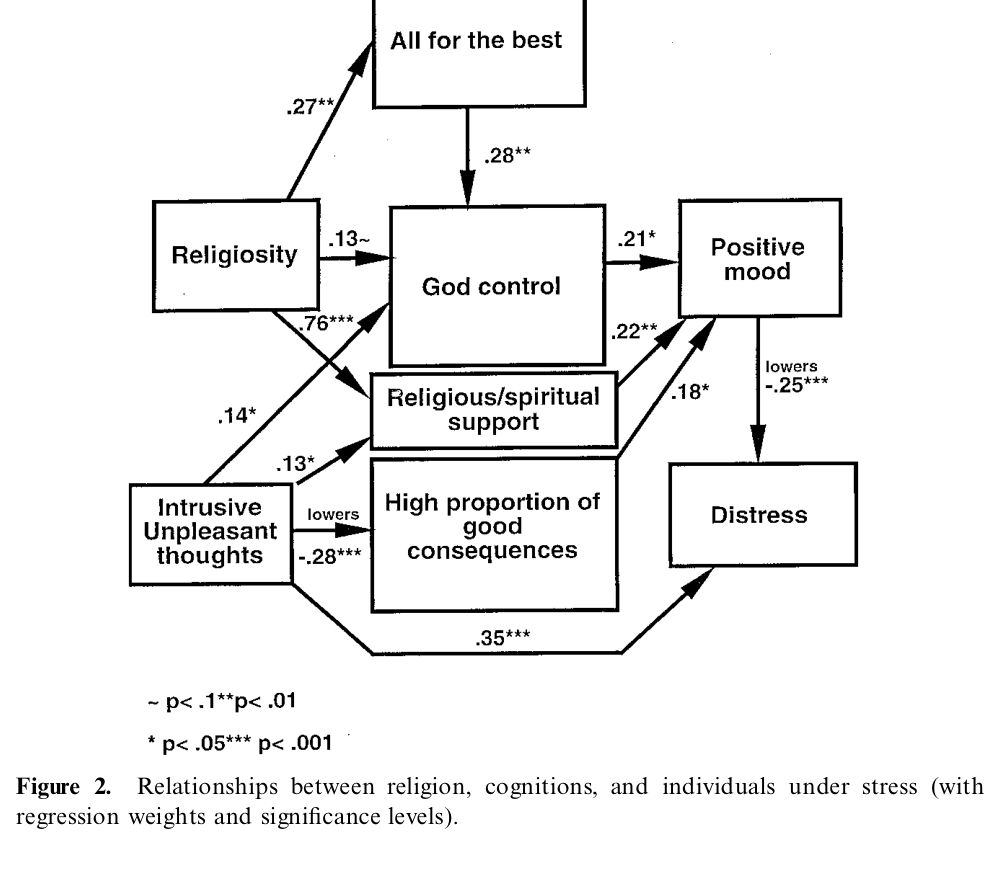
The correlations in Table 2 were used to test the causal pathway model outlined in Figure 1. However as noted, only the G-d control variable was retained from the causal attributional measures since they did not related significantly to other variables. Using structural equation modelling (AMOS), the initially-hypothesised model shown in Figure 1 produced unacceptably large goodness-of-fit statistics (X2=43.5, d.f.=12, p=.000, X2/d.f.>2; Normed Fit Index (NFI)= .772). Changes were made by deleting non-significant pathways, and by altering relationships between variables to make the best theoretical sense. The two main changes of this type were first, that intrusive unpleasant thoughts were best placed as antecedents rather than outcomes. A model in which they remained as outcomes, as originally hypothesised, had goodness-of-fit statistics similar to those of Figure 2. However without more data we could not justify it theoretically, since intrusive unpleasant thoughts related positively to the religious coping cognitions. The second main change was the deletion of the direct causal pathways between distress outcome and all of the coping cognitions variables. Figure 2 shows the best-fit model with regression weights. Goodness-of-fit statistics were satisfactory: X2 = 22.74, d.f.=16, X2/d.f.= 1.42; Normed Fit Index (NFI)=0.881).
Causal pathway models based on the separate Protestant and Jewish data suggested no noteworthy differences from the model shown in Figure 2.
INSERT FIGURE 2 ABOUT HERE
Discussion
How did the hypotheses and research questions fare? As hypothesised, religiosity was associated with the religiously-based cognitions, but these were not in turn directly associated with lowered distress. The only connection between these religious coping cognitions and lowered distress was that they were associated with raised positive affect, which in turn was associated with lowered distress. If the religiously-based cognitions studied here are involved in the association between religiosity and lower distress, then it might be via this route. However the route is speculative since we cannot be confident about the direction of all the causal links, for instance that positive affect lowers distress.
There was only weak, partial support for the second hypothesis about consequences and attributions and their relations with distress. The perception of positive consequences did not relate directly to lowered distress. Like the religious cognitions, the perception of good consequences related to positive affect, and thus might have had an indirect distress-lowering effect. External, unstable and specific attributions did not relate to either positive affect or to distress (or to any other measures). Brewin (1988) has concluded that there is actually little or no evidence for the possibility that internal, stable, global attributions play a role in the onset of depression, as opposed to being a symptom or maintenance factor. It was largely the role of attributions in onset that was tested here and we discovered no evidence at variance with Brewin's conclusions.
Thirdly, we predicted that the consequence and attributional measures would also mediate the relationship between religiosity and distress. In fact neither the consequences nor the attributional measures related to religiosity. This prediction was speculative and although there has been some work suggesting links between religiosity and patterns of causal explanation, none map precisely onto the specific associations between religiosity and distress hypothesised for this study. The consequences cognitions seemed to be involved in a separate route to coping, independent of religiosity.
An exploratory aspect of the work was to examine the moderating role that positive affect might have on distress. In fact the best-fitting causal pathway model differed from the hypothesised model chiefly in that the cognition variables had no direct relationship with distress, only with positive affect.
The two major differences between the initial causal pathway mode in Figure 1, and the best-fit model in Figure 2, were caused by the associations indicating that distress was not directly lowered by the religious coping cognitions, and that intrusive unpleasant thoughts should be considered outcomes rather than antecedents. This shift resulted from our view that without more data, we could not explain how religious coping cognitions could cause intrusive unpleasant thoughts. We could however argue that intrusive unpleasant thoughts might stimulate religious coping cognitions (McIntosh, 1995). We had some expectation that religion and its beliefs might directly lower distress, and indeed unpleasant thoughts. However the data suggest a different set of causal pathways. Rather than religious coping cognitions lowering intrusive unpleasant thoughts and distress, it looks as if intrusive unpleasant thoughts stimulate religious coping cognitions from any repertoire established by religious activities, as MacIntosh (1992) has suggested. To the extent that these cognitions are called into play, positive mood is evoked, and to the extent that positive mood is evoked, distress is lowered. Thus any effect of religious cognitions in combating unpleasant thoughts was outweighed by a reverse effect: unpleasant thoughts appear to have stimulated religious coping beliefs - which were a source of positive affect, and indirectly lowered distress. Any lowering effect of religion on distress is thus indirect, via cognition and mood.
We have suggested in Figure 2 that positive mood may lower distress, though of course the reverse may be equally possible. Little is known about the direct effects of positive and negative mood states upon each other. Clark & Watson (1988) suggest that positive and negative mood are driven independently of each other by daily events: positive affect "ebbs and flows with the tide of events", while negative affect "crashes on us in times of trouble, only to disappear when the storm is over" (p.305). Several authors, however, have argued that mood and distress states are not directly driven by events but, rather, cognitive factors intervene. Further, Brown, Bifulco & Andrews (1990), MacLeod & Byrne (1996) and Needles & Abramson (1990) support the suggestion that a cognitively-driven improvement in mood may have a direct lowering effect upon distress. Our evidence suggests that this may be the case in this study.
Another noteworthy feature of the empirically-based model in Figure 2 is the good consequences measure. This proved to be independent of the more global measure of seeing that ones troubles are all-for-the-best, and it related differently to other variables: it was independent of religion, and inversely related to intrusive unpleasant thoughts. The distinction between seeing specific consequences and general consequences is reminiscent of Williams' (1997) argument that specific and general memories play different roles vis-à-vis emotion and the emotional disorders. Williams suggests that degree of trauma and distress is associated with fewer specific memories. In the present study, intrusive unpleasant thoughts, which were associated with distress, were associated with smaller proportions of positive specific consequences, such as memories of good outcomes and hopes for the future. Our data in relation to Williams' ideas suggest that the interplay between specific cognitions, distress and intrusive unpleasant thoughts deserves further attention. We have suggested particular causal directions of effects but do not wish to exclude other possibilities. There was, however, one similarity between good consequences and the religious coping cognitions: both were associated with positive mood, and any distress-relieving effects appeared to operate indirectly, via improved mood.
Figure 2 is empirically-driven, but some of the suggested directional causal associations may not be warranted. We have made the best suggestions that we can in the light of the evidence and existing theory about what we think are the salient effects in the present study. The probability of bi-directional effects cannot be excluded. Thus those who are more cheerful may be better able to access comforting thoughts from a religiously-based repertoire, stress-related intrusive unpleasant thoughts may limit access to thoughts of specific positive consequences, and distress may lower positive mood - to indicate the most plausible alternative causal possibilities, which cannot be ruled out in a cross-sectional study. However we have examined these possibilities by partialling out the effects of positive mood, intrusive unpleasant thoughts and distress, and they had no appreciable effects.
To focus on one set of links - those surrounding perceived G-d control - we could consider more elaborate (alternative) interpretations. It has been suggested that people may be less likely to associate G-d with bad outcomes (Lupfer et al., 1992). This might be explained by putting together the self-serving bias (Zuckerman, 1979), the just world hypothesis (Lerner, 1980), and the suggestion of links between religion, guilt and self-esteem (Hood, 1992). The chain of reasoning might be: "If I feel bad now, I am not going to blame G-d, since this would mean I agree that G-d might be punishing me for being a bad person. Since I do not want to agree that I am bad, I am not going to say that G-d has anything to do with it". This kind of effect might account for some of the associations between religion, perceived G-d control and positive mood. It is also possible that some individuals may see G-d as a perceived cause for their sufferings, and instead of rejecting G-d as a cause, feel unworthy and unhappy as a result (Pargament & Brant, 1998). Our evidence does not offer much support for this having been a dominant effect, but it might have weakened the associations between religiosity, perceived G-d control and positive mood. Other effects at work might include the possibility that some individuals perceive a high degree of G-d control, coupled with a belief that all will work out ultimately for the best. This could account for the association between perceived G-d control and the overall all-for-the-best measure. And finally we must consider the possibility that perceived G-d control is more likely for some types of events than others. This could account for the tenuousness of the relationship between religiosity and G-d control.
Apart from the difficulties of interpreting direction and nature of causality, there are other limitations of the study. Better attention needs to be given to individual differences in religious and coping styles. Intrinsic religiosity has been highlighted in previous work as a strong candidate for a religiously-related stress-buffering factor. Extrinsic religiosity has been associated with poorer mental health (Batson et al., 1993). Pargament has identified three styles of religious coping: deferring, self-directing and collaborative (Pargament, Kennell, Hathaway, Grevengoed, Newman & Jones, 1988). For pragmatic reasons, we used a combined measure of religious activity but appreciate that a full account of religious coping must take fuller account of individual differences.
A related possibility is that, as suggested, there are negative effects of religiosity lurking among the data, masked by other effects. For example, Edmunds & Hooker (1992), and Wallston, Malcarne, Flores, Hansdottir, Smith, Stein, Weisman & Clements (in press) have recorded associations between religiosity and distress, for example that sometimes the use of prayer may be a desperate last resort, associated with catastrophizing and hopelessness. Religiously-based thoughts associated with distress might include “G-d is punishing me”, or “G-d does not care about me” (Pargament & Brant, 1998; Smith, 1999). These observations differed from ours, and involved those suffering from specific types of stress. To clarify the different effects, more precise distinctions need to be made, for example in assessing perceptions of G-d control - as Pargament et al. (1988), and Wallston et al. (1988) have done.
A possibly problematic feature of the methodology is thrown up by the causal pathway analysis. The move of intrusive unpleasant thoughts from the role of outcomes to antecedents was suggested because intrusive thoughts related positively to religious coping cognitions. Perhaps, as suggested, Intrusive unpleasant thoughts stimulated religious coping cognitions (McIntosh, 1995). But we did not have sufficiently precise measures to determine whether other causal pathways were possible. As discussed, we could not determine whether some religious thinking is associated with negative outcomes (Pargament & Brant, 1998; Smith, 1999) since we had no measures of cognitions such as “G-d does not care about me”. Such thinking is very likely associated with religiosity, and is likely involved in a spiral of deteriorating mood and brooding about the unhelpfulness of G-d. However we did not have measures to look at these relationships.
Another methodological limitation is that in the initial screening those scoring in the middle of the self-rated religiosity scale were for several reasons excluded from the study. Although this scale was not used as the basis for any of the analyses reported, it may nevertheless have resulted in some biasing of the sample, which future research could rectify.
A final point for comment is the similarity between Protestants and Jews on the measures of religion, cognition and outcome. There are some suggestions of different prevalences of psychiatric disorders in the two groups, and some differences in the importance of different causal factors (Loewenthal et al., 1995, 1997a, 1997b; Levav, Kohn, Golding & Weissman, 1997). This study however produced no noteworthy evidence of Protestant-Jewish differences in distress, and (perhaps paralleling this) there were no noteworthy Protestant-Jewish differences in the cognitions studied here. Our research design enabled us to ensure that levels and types of stress were similar in the two groups of participants. We feel confident that there were genuine commonalities between the two religious traditions in the cognitive aspects of coping.
There are features of this study which deserve emphasis. First, although the design involved cross-sectional measurement, we have incorporated features of the important methodologies developed by Brown & Harris (e.g. 1978, 1989), which ensured that reported life-events and difficulties were prior to current mood and symptoms, and thus could be causal or maintenance factors. Contextual stress measurement was also used. These features have been argued to overcome some of the traditional difficulties of cross-sectional and retrospective studies. Therefore although we wish to be cautious about the directions of causality suggested, we also wish to emphasise that our research design lends some support in terms of temporal ordering: stress was determined to be prior to the outcome measures (positive mood and distress), and the coping-related cognitions were explicitly related to coping with the prior event or stressor. The main shortcoming in the design was the failure to assess religiosity prior to the stressor. This weakens our direction of causality suggestions as far as religiosity is concerned, since the measurement of religiosity does not allow us to position it temporally in relation to the other variables. Also we could not look at religious change in relation to outcome.
Other important features of the study include the separation of positive mood and negative mood (distress) measurement, in line with growing body of suggestions that these features of emotion need to be considered independently. A final feature of the study was the range of measures of religion-related features of coping. There are directions in which these could be made more precise, and this will in turn improve understanding of ways in which aspects of religion may be related to worse and better outcomes in individuals under stress.
In conclusion, this study offers suggestions about some roles played by religion in mediating between stress and distress, as well as mediating pathways that were independent of religion. The study offers suggestions regarding which religious beliefs and ideas might be effective in stress-moderating, and how these beliefs and ideas might achieve their effects. In particular, the interplay of cognition and emotion in comfort deserves further study.
References
Allport, G.W. & Ross, J.M. (1967) Personal religious orientation and prejudice. Journal of Personality and Social Psychology, 5, 432-443.
Batson, C.D. (1976) Religion as prosocial: agent or double agent. Journal for the Scientific Study of Religion, 15, 29-45.
Batson, C.D., Schoenrade, P.A. & Ventis, W.L. (1993) Religion and the Individual: A Social-Psychological Perspective. Oxford: Oxford University Press.
Bedford, A., Foulds, G.A. & Sheffield, B.F. (1976) A new personal disturbance scale. British Journal of Social and Clinical Psychology, 15, 387-394.
Bergin, A. (1991) Values and religious issues in psychotherapy and mental health. American Psychologist, 46, 394-403.
Brewin, C.R. (1988) Cognitive Foundations of Clinical Psychology. Hove and London: Erlbaum.
Brown, G.W., Bifulco, A. & Andrews, B. (1990) Self-esteem and depression: 4. Effect on course and recovery. Social Psychiatry and Psychiatric Epidemiology, 25, 244-249.
Brown, G. & Harris, T.O. (1978) The Social Origins of Depression. London: Tavistock.
Clark, D.M. & Teasdale, J.D. (1982) Diurnal variation in clinical depression and accessibility of positive and negative experiences. Journal of Abnormal Psychology, 91, 87-95.
Clark, L.A. & Watson, D. (1988) Mood and the mundane: Relations between daily life events and self-reported mood. Journal of Personality and Social Psychology, 54, 296-308.
Edmonds, S. & Hooker, K. (1992) Perceived changes in life meaning following bereavement. Omega - Journal of Death and Dying, 25, 307-318.
Fava, G.A., Rafanelli, C., Cazzaro, M., Conti, S., & Grandi, S. (1998). Well-being therapy: A novel therapeutic approach for residual symptoms of affective disorders. Psychological Medicine, 1998,
Furnham, A. & Brown, L.B. (1992) Theodicy: a neglected aspect of the psychology of religion. International Journal for the Psychology of Religion, 2, 37-46.
Gotlib, I.H. & Hammen, C.L. (1992) Psychological Aspects of depression: Toward a cognitive interpersonal interpretation. Chichester: Wiley.
Hood, R.W. (1992) Sin and guilt in faith traditions: Issues for self-esteem. In J. Schumaker (ed) Religion and Mental Health. Oxford: Oxford University Press.
Janoff-Bulman, R. (1979) Characterological versus behavioural self-blame: Inquiries into depression and rape. Journal of Personality and Social Psychology, 37, 1798-1809.
Klonoff E.A. & Landrine H. (1994) Culture and gender diversity in commonsense beliefs about the causes of six illnesses. Journal of Behavioural Medicine, 17, 407-18.
Lazarus, R.S. & Folkman, S. (1984) Stress, Appraisal and Coping. New York, Springer.
Lerner, M.J. (1980) The Beliefs in a Just World: A Fundamental Delusion. New York: Plenum.
Levav, I., Kohn, R., Golding, J.M., Weissman, M.M. (1997) Vulnerability of Jews to affective disorders. American Journal of Psychiatry, 154, 941-947.
Levin, J.S. (1994) Religion and health: Is there an association, is it valid, and is it causal? Social Science and Medicine, 38, 1475-1482.
Loewenthal, K.M. (1992) Melancholy, Depression and Judaism. International Journal for the Psychology of Religion, 2, 101-108.
Loewenthal, K.M. & Cornwall, N. (1993) Religiosity and perceived control of life events. International Journal for the Psychology of Religion, 3, 39-46.
Loewenthal, K., Goldblatt, V., Gorton, T., Lubitsh, G., Bicknell, H., Fellowes, D. & Sowden, A. (1995) Gender and depression in Anglo-Jewry. Psychological Medicine, 25, 1051-1063.
Loewenthal, K.M., Goldblatt, V., Gorton, T., Lubitsh, G., Bicknell, H., Fellowes, D., & Sowden, A. (1997a) The costs and benefits of boundary maintenance: stress, religion and culture among Jews in Britain. Social Psychiatry and Psychiatric Epidemiology, 32, 200-207.
Loewenthal, K.M., Goldblatt, V., Gorton, T., Lubitsch, G., Bicknell, H., Fellowes, D., & Sowden, A. (1997b) The social circumstances of anxiety and its symptoms among Anglo-Jews. Journal of Affective Disorders, 46, 87-94.
Lupfer, M.B., DePaola, S.J., Brock, K.F. & Clement, L. (1994) Making secular and religious attributions - the availability hypothesis revisited. Journal for the Scientific Study of Religion, 33, 162-171.
MacLeod, A.K. & Byrne, A. (1996) Anxiety, depression, and the anticipation of positive and negative experiences. Journal of Abnormal Psychology, 105, 286-289.
MacLeod, A.K., Rose, G.S. & Williams, J.M.G. (1993) Components of hopelessness about the future in parasuicides. Cognitive Therapy and Research, 17, 441-455.
Maton, K.I. (1989) The stress-buffering role of spiritual support: cross-sectional and prospective investigations. Journal for the Scientific Study of Religion, 28, 310-323.
McIntosh, D. (1995) Religion-as-Schema, with implications for the relation between religion and coping. International Journal for the Psychology of Religion, 5, 1-16.
Myers, D.G. & Diener, E. (1995) Who is happy? Psychological Science, 6, 10-19.
Needles, D.J. & Abramson, L.Y. (1990) Positive life events, attributional style, and hopefulness: Testing a model of recovery from depression. Journal of Abnormal Psychology, 99, 156-165.
Paloutzian, R.F. (1981) Purpose in life and value changes following conversion. Journal of Personality and Social Psychology, 41, 1153-1160.
Pargament, K.I. & Brant, C.R. (1998) Religion and coping. In H.G.Koenig (editor) Handbook of Religion and Mental Health. New York: Academic Press.
Pargament, K.I., Kennell, J., Hathaway, W., Grevengoed, N., Newman, J. & Jones, W. (1988) Religion and the problem-solving process: Three styles of coping. Journal for the Scientific Study of Religion, 27, 90-104.
Pennebaker, J.W. (1985) Traumatic experience and psychosomatic disease: exploring the roles of behaviour inhibition, obsession and confiding. Canadian Psychology, 26, 82-95.
Prudo, R., Harris, T.O. & Brown, G.W. (1984) Psychiatric disorder in an urban and in a rural population 3: social integration and the morphology of affective disorder. Psychological Medicine, 14, 327-345.
Sanua, V.D. (1989) Studies in mental illness and other psychiatric deviances among contemporary Jewry: a review of the literature. Israel Journal of Psychiatry and Related Sciences, 1989, 26, 187-211.
Shmool, M. & Cohen, F. (1990) British Synagogue Membership in 1990. London: Research Unit of the Board of Deputies of British Jews.
Smith, C.A. (1999) Personal communication.
Staples, C.L. & Mauss, A.L. (1987) Conversion or commitment? A reassessment of the Snow & Machalek approach to the study of conversion. Journal for the Scientific Study of Religion, 26, 133-147.
Stratton, P., Heard, D., Hanks, H.G.I., Munton, A.G., Brewin, C.R. & Davidson, C. (1986) Coding causal beliefs in natural discourse. British Journal of Social Psychology, 25, 299-313.
Wallston, K., Malcarne, V., Flores, L., Hansdottir, I., Smith, C.A., Stein, M.J., Weisman, M.H., & Clements, P.J. Does God determine your health? The God Locus of Health Control Scale. (In press).
Watson, D., Clark, L.A. & Tellegen, A. (1988) Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063-1070.
Williams, J.M.G. (1997) Cry of Pain: Understanding Suicide and Self-Harm. Harmondsworth: Penguin.
Williams, J.M.G., Watts, F.N., MacLeod, C. & Mathews, A. (1988) Cognitive psychology and emotional disorders. Chichester: Wiley.
Williams, J.M.G. & Hargreaves, I.R. (1994) Neuroses: Depressive and Anxiety Disorders. In A.A.Lazarus & A.M.Colman (eds) Abnormal Psychology. London: Longman.
Worthington, E.L.,Jr., Kurusu, T.A., McCullough, M.E. & Sandage, S.J. (1996) Empirical research on religion and psychotherapeutic processes and outcomes: A 10-year review and research prospectus. Psychological Bulletin, 119, 448-487.
Zinnbauer, B.J., Pargament, K.I., Cole, B., Rye, M.S., Butter, E.M., Belavich, T., Hipp, K.M., Scott, A.B. & Kadar, J.L. (1997) Religion and spirituality: Unfuzzying the fuzzy. Journal for the Scientific Study of Religion, 36, 549-564.
Zuckerman, M. (1979) Attribution of success and failure revisited, or: the motivational bias is alive and well in attribution theory. Journal of Personality, 47, 245-287.
Author notestc
Kate Miriam Loewenthal, Andrew MacLeod, Vivienne Goldblatt, Guy Lubitsh, and John Valentine, Department of Psychology, Royal Holloway University of London.
This project was supported by the Wellcome Trust (Grant No. 038946/Z/93/Z).
The authors would like to thank Helen Bicknell, Tessa Gorton, Tracey Francis and Paul Egbers for their assistance with interviewing and analysis, Tirril Harris and Bernice Andrews for advice on the LEDS, and Chris Brewin for advice on design. The authors would also like to thank the participants who took time out during very difficult periods in their lives to answer our questions about how they coped, and Craig Smith and several anonymous reviewers for their very careful and constructive analysis of earlier drafts of this paper.
Correspondence concerning this article should be addressed to Kate Miriam Loewenthal, Psychology Department, Royal Holloway University of London, Egham, Surrey TW20 OEX, UK.
Table 1. Frequencies of different types of stress among Protestants and Jews.
|
Type |
Protestant n=68 |
Jewish n=58 |
X2 |
|
Finance, Employment |
52% (35/68) |
38% (22/58) |
2.04 n.s. |
|
Illness |
52% 35/68) |
58% (30/58) |
<1 n.s. |
|
Relationships, family |
36% (24/68) |
50% (29/58) |
2.08 n.s. |
Table 2: Inter-correlations between religion, cognition and mood measures.
|
|
Religiosity |
All for The best |
G-d control |
Religious (spiritual) support |
Proportion of good consequences |
Positive mood |
Distress |
Intrusive unpleasant thoughts |
|
Religiosity |
- |
|
|
|
|
|
|
|
|
All for the Best |
.29** |
- |
|
|
|
|
|
|
|
G-d control |
.30* |
.37** |
- |
|
|
|
|
|
|
Religious (spiritual) Support |
.80*** |
.15 |
.18 |
- |
|
|
|
|
|
Proportion Of good consequences |
.17 |
.17 |
.00 |
.16 |
- |
|
|
|
|
Positive mood |
.37*** |
.29* |
.21* |
.27** |
.22* |
- |
|
|
|
Distress |
.00 |
-.07 |
-.16 |
.02 |
-.18 |
-.27*** |
- |
|
|
Intrusive Unpleasant thoughts |
.22* |
-.04 |
.26* |
.27** |
-.24* |
-.02 |
.40** |
- |
Notes 1): * p<.05, ** p<.01, ***p<.001 (all two-tailed probabilities).
2) Further, partial correlations were computed, partialling out the effects of i) positive mood ii) intrusive thoughts and iii) distress. The coefficients were of the same order as those shown above and are therefore not included.
Figure 1. Hypothetical relationships between religion, cognitions, and outcomes in individuals under stress.
Figure 2. Relationships between religion, cognitions, and individuals under stress (with regression weights and significance levels).