SYNOPSIS
This study found similar prevalence of case depression among men as among women in a sample of 339 Jews affiliated to orthodox synagogues (157 men and 182 women). There were significant gender differences in several social-situational factors and symptoms, mostly in the direction that would suggest that case depression would be higher among women than among men. That this was not so is suggested to be the result of the cultural milieu: social factors that have been found to be associated with depression in other groups of people did not function as risk or vulnerability factors among the Jews studied. In particular, the evidence indicates the importance of specific cultural-religious values in contributing towards the prevalences that were observed. These values included the esteem attached to women's central role in family management, and the low use of alcohol and suicide as escape routes from depression.
INTRODUCTION
Is depression a woman's illness? Some work has suggested a higher prevalence of depression among women than among men. This however may not be culturally or historically universal, and it is not clear whether gender differences arise from social-situational factors, gender-linked biological differences, or both. This paper examines i) gender differences in prevalence of case depression, and ii) some causal and risk factors, among Jews affiliated to orthodox synagogues in the London area. We look at whether social-situational factors and individual differences were related both to case depression and to gender, and could therefore account for the prevalences of depression that were observed.
The Jews studied were recruited from orthodox synagogue membership lists. It is estimated that most Jews maintain synagogue affiliation because of the importance attached to Jewish burial which is normally guaranteed to synagogue members and their families (Waterman & Kosmin, 1986). Stable marriage is fairly normative among Jews, with a strong focus on family life, involving the religious calendar, rites of passage, and the care, education and upbringing of children. Types of employment and social attitudes and behaviour norms differ from those of the general population (e.g.Kosmin & Grizzard, 1975; Kosmin & Levy, 1983; Waterman & Kosmin, 1986). Some scientific attention has been given to the possibility of lower levels of alcoholism (Ball & Clare, 1990) and physical violence (Moeller, Bachman & Moeller, 1993) among Jews than among other groups. Jews are, of course, a minority group and at risk of racist abuse and other disadvantages of minority group status. Many members of the Jewish community (particularly the strictly-orthodox) are survivors of the Nazi holocaust, or the children or grandchildren of survivors, and extremely sensitive to the issue of anti-semitism.
Evidence on gender differences in depression
Referrals: although referral rates do not necessary reflect prevalences, they may prompt examination of prevalence. Evidence from referrals for treatment suggested that women are more likely to seek treatment for psychological illnesses than men, especially for depressive disorders (e.g. Brown & Harris, 1978; Cochrane, 1983, 1993; Paykel, 1991), and that different aspects of social support relate to recovery (Brugha & Bebbington, 1990). However gender differences in referral rates vary with cohort and marital status. For marital status, the effects appear to be that married men appear to be relatively more 'protected' from depression than are not-now-married men; this effect has not been so marked for women and sometimes (for women) the reverse effect has been reported. There are cohort effects on gender differences in referral, such that referral rates for men may be similar to, or higher than that of women (Lowe & Garrat, 1959; Cochrane, 1983).
On psychometric measures of depressed mood and symptoms, women have been said to score higher than men (Cochrane, 1993). However, several studies do not show any such differences (Zuckermen & Lubin, 1963; Hong & Grambower, 1986; Beck & Steer, 1987; Steer, Beck & Brown, 1989; Loewenthal, Gorton & Goldblatt, in preparation). Depressed mood measures do not however provide direct evidence about depressive illnesses as such.
Prevalence in the community: Work on prevalence of depression in community samples has not always attended to gender differences (e.g. Brown & Harris, 1978; Cochrane, 1983). Brown & Harris (1989) suggest that depression is less commonly found among men than among women, "at least in urban settings" - implying that in non-urban settings, men may be as likely to be depressed as women. There are a number of community studies which have examined gender differences i) in prevalence of depression in different communities, ii) in the causes of depression, and iii) in the handling of depression, including seeking help. Such studies suggest that relations between gender and depression vary with age/ marriage/ parity or cohort, and with whether the community is 'traditional'. Carta, Carpiniello, Morosini & Rudas (1991) in a Sardinian community study showed no gender differences in depression. Another study, among Jews in London carried out three years prior to the current study, drawn from similar synagogue membership lists, found men more depressed than women, with husbands more depressed than their wives. (Loewenthal, 1993). Community studies that report depressive illness as more likely in women than men tend to have been in non-traditional societies e.g. Finland (Lehtinen, Lindholm, Veijola & Veisanen, 1990), Sweden (Rorsman, Grasbeck, Hagnell & Lanke, 1990), New Zealand (Joyce, Oakley-Browne, Wells & Bushnell, 1990) (however in this study, in the youngest cohort, men had a higher prevalence than the women), the UK (e.g Bebbington, Katz, McGuffin & Tennant, 1989) and the USA (e.g. Murphy & Leighton, 1989). In the New Zealand study just mentioned (Joyce et al 1990), there was a suggestion that there might be generational, age or cohort effects in the differential prevalence of depression among men and women. Women had higher prevalence of depression than men in the older cohorts, but the younger men were more likely to be depressed than the younger women. Silverstein & Perlick (1991) reported historical changes in gender differences in depression in the USA. Such differences were high among cohorts that reached adolescence during periods of increasing opportunity for female achievement, but were not significant in periods of stable or decreasing opportunities for women. Other reports have suggested that gender differences are only apparent once women have married and/or had children (Gater, Dean & Morris, 1989; Bebbington, Dean, Der & Hurry, 1991).
Thus in community and other samples there is by no means a universal tendency for women to emerge as more likely to be depressed than men. Gender differences in depression may be related to whether or not the society or group under study is 'traditional'. There are cohort and age effects, the latter possibly resulting from the effects of marriage and/or parity.
Gender and depression: explanations.
Explanations of gender differences in mental illness have generally been concerned with explaining why women are more likely to be depressed than men. Although this may not always be so, explanations for greater likelihood of female depression are of relevance to the understanding of causal processes in depression in both men and women.
Biological. Paykel (1991) suggested that biological explanations are plausible, although hard to test. Calloway & Dolan (1989) have attempted to deal with some of the methodological and interpretive difficulties in this field. They conclude that the endocrine functioning patterns characteristic of depression are influenced by environmental factors (stressors). They present no evidence on 'innate' gender-linked differences in the aspects of endocrine functioning associated with depression. Cochrane (1993) concluded that there is no firm evidence to support a biologically-based underpinning for sex differences in depression. Jenkins' (1985) study suggested some sex differences in minor psychiatric morbidity and illness behaviour among young British adults (aged 20-35) when environmental differences had been minimised. Harris, Surtees & Bancroft (1991) suggested that biological factors - particularly hormonal changes related to contraceptive use, pregnancy, birth and lactation - may need to be invoked to explain findings that male-female differences in depression are greatest at life stages when reproductive roles diverge the most (Gater et al, 1989; Wilhelm & Parker, 1989; Bebbington, 1991). Thus age, marriage and parity effects on gender differences in depression may be confounded with each other and with biological factors.
Social-situational. Differences in the social situations of women and men may explain gender differences in depression. Such explanations include -
i) Women are in a less powerful position than men, which leads them to develop styles of coping that are already akin to depression, such as compliance, passivity and helplessness (Cochrane, 1983).
ii) Marriage and homemaking are more costly and less beneficial to women than to men. Rosenfield (1992) suggested that housework has a lowering effect upon wellbeing. The burdens of housework, homemaking and caring all tend to fall on women, while men may gain benefits from marriage (such as support, status and comfort) with incurring such costs (Kessler & McLeod, 1984; Cochrane, 1993; Hobfoll, 1991)). Bebbington (1991) and Gater et al (1989) reported effects of marriage and parity in explaining gender differences in depression. Brown & Harris (1978) reported that women with several young children to care for were more vulnerable to depression following loss than women with lighter family responsibilities. This finding however may be cohort-specific and Loewenthal & Goldblatt (1993) suggested some positive effects of family size on mental health. Prestige and resources may be more available to women in traditional societies engaged in homemaker and childcare roles.
iii) Women are less likely to be gainfully employed, and employment has been suggested as generally protective where it provides a social support systems, income, status and other resources (Gove, 1972; Brown & Harris, 1978; Rosenfield, 1992; Cochrane, 1993). However employment may contribute to overload where mothers are concerned: Brown & Bifulco (1990) reported higher risk of depression among full-time (but not part-time) working mothers compared to non-workers.
iv) Stress levels for women and men differ. Women may suffer more depression-inducing stress. Hobfoll (1991) found Israeli women more likely than Israeli men to report depressed mood, the result of role overload. Newman (1986) reported that hardships had an equal effect in both men and women, in leading to depressive syndrome; however women were found to report more of certain hardships than men.
Responses to stress. Gender differences in depression may be explained by differences in ways of handling stress and psychological pain. These may be a result of social-situational differences, but the focus is on individual differences rather than the social circumstances that may cause these to arise. Explanations of this third type include -
i) Women and men differ in their habits of thinking. Episodes of depression may be prolonged and possibly more severe if the sufferer engages in ruminating (Nolen-Hoeksema, 1987): focusing on symptoms and their possible causes and consequences, amplifying depressed mood. Women are more likely to ruminate than men, possibly as a result of powerlessness, particularly lack of resources. Men are more able and likely to engage in distracting behaviour, dampening depressed mood.
ii) Men may be more reluctant or less able to seek help for depression, which is also less likely to be diagnosed among men than among women given similar symptoms (Potts, Burnam & Wells, 1991).
iii) Men who attempt suicide are more likely to actually kill themselves than women. This leaves more depressed women to be diagnosed as suffering from depression;
iv) Distressed men may develop psychopathologies other than depression. In many societies, alcohol consumption is more likely among men than among women as a response to stress and distress (Robbins & Martin, 1993; Golding, Burnam & Wells, 1990; Berger & Adesso; 1991). Ball & Clare (1990) explained high referral rates for London Jewish men in terms of lower use of alcohol by depressed Jewish men.
v) Depressed men may simply fail to report depression, perhaps to maintain self-esteem (Vredenburg, Krames & Flett, 1986;
Wilhelm & Parker, 1989).
This third set of explanations is thus that depressed men may be more likely than depressed women to develop a syndrome that is not primarily depressive in its presenting symptoms. They may be less likely to seek help, and they may be less likely to be recognised as depressed by mental health professionals.
Aims of the present study. This study examined case depression and some of its causes in Jewish men and women affiliated to orthodox synagogues in the London area. The primary question was whether case depression was more likely in the women than in the men studied. The evidence reviewed above suggests that gender differences in prevalence rates might be low since the groups studied were traditional. Cultural factors may be associated with a raised prevalence of depression among men: among Jews, admitting to depressed mood may be more culturally acceptable among men than it is in other groups, and violence and alcohol consumption less normative and less acceptable (Ball & Clare, 1990; Moeller, Bachmann & Moeller, 1993).
The explanations reviewed above could be examined in the light of the data collected. Specifically, there were sufficient data to examine the following:
1. Differences between men and women in social circumstances:
a. lack of confiding (close, supportive) relationship;
b. homemaker role only;
c. not in paid employment;
d. married;
e. parity (having one or more children);
f. large family (three or more children; we used this criterion, following Brown & Harris (1978) but did not exclude children over 14 since it was normative among the groups studied for parents to maintain close ties and financial and other responsibility for adult children);
g. stress: three contextual measures were used: presence of a provoking agent, overall number of events and difficulties, and presence of specifically economic threats and difficulties.
2. Differences between men and women in responses to stress were examined by comparing frequencies of selected symptoms. The following were examined:
a. inefficient thinking, concentration and brooding (rumination more likely among women than men);
b. evidence of medical consultation;
c. self-deprecation and lack of self-confidence (women more powerless);
d. drinking;
e. suicidal plans and thoughts of death;
f. increased irritability, shouting and hitting;
g. hostility rated as expressed during interview.
This study examined
i) the relations between gender and case depression among Jews.
ii) Gender differences in social-situational factors and stress responses.
iii) Whether any such social-situational factors were related to case depression.
METHOD
Brown & Harris (1978, 1989) pioneered contextual methods of assessing contextual stress, which were used in the current study. Contextual stress has been suggested to be causally-related to depression and to other illnesses (Brown & Harris, 1989).
Subjects
Subjects were recruited by first writing to and second, telephoning one household in five from lists of members of traditional and strictly orthodox synagogues in the greater London area. Available adult household members were asked if they would be interviewed. In 259/460 (58.5%) of households contacted, at least one adult agreed to be interviewed. In 70 of these households, two or more adults were interviewed, usually husband and wife. It appeared that retired or unemployed people may have been more willing and available to be interviewed than others, which may account for the fairly high mean age of the sample. The fairly low response rate may be associated with some bias in the sample interviewed, which may not be representative of the groups from which they were drawn. Although response rates were low, they were considered high in relation to those reported by other workers attempting to study orthodox-affiliated Jews (Ingram & Lowe, 1989; Shmool & Miller, 1994). In order to undertake this study, it was necessary to obtain approval and consent for the investigation from rabbis and communal leaders; prospective interviewees were prepared to accept this as a sign of our trustworthiness. The most common reason for refusal to participate was 'too busy'.
Altogether 339 subjects were interviewed: 157 men and 182 women.
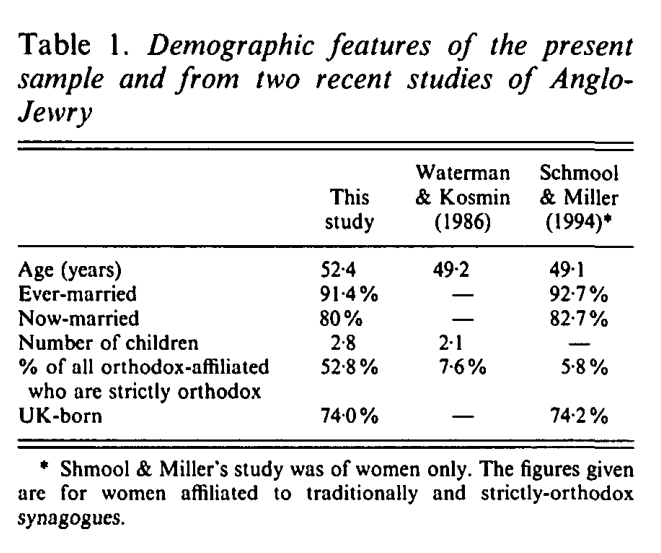
Table 1 shows characteristics of the sample, which has very similar characteristics to those of other recently-studied samples of Anglo-Jewry with respect to age, marriage, and whether UK-born. However, synagogue affiliation differs; we aimed for approximately equal numbers of strictly and traditionally-orthodox-affiliated subjects so as to make comparisons on the basis of religious affiliation, and to increase the numbers of subjects with large families (large families being common among the more strictly orthodox). Waterman & Kosmin, and Shmool & Cohen (1990) suggest about four to five times as many traditional-orthodox as strictly-orthodox affiliates. Thus, due to the inclusion of a high proportion of strictly-orthodox affiliates, family size was larger in this sample compared to Waterman & Kosmin's figure of 2.1.
Table 1
Note that 'orthodox' refers to synagogue affiliation and not to religious observance, which was found to vary quite widely among the subjects interviewed. Some effects of orthodoxy of affiliation were briefly examined in this paper (religion has been widely suggested as having a stress-buffering effect (e.g. Maton, 1989; Levin, 1994; Loewenthal, 1995).
The interviews were conducted in 1991-3, during a period of economic recession. There appeared to be considerable amounts of stress associated with these economic conditions; some subjects had been running small businesses and had become bankrupt. Others had suffered redundancy. Others - teachers in religious Jewish schools which receive little or no state aid and which depend on charitable support - had not been paid for several months and were heavily in debt.
Measures and sampling
One household in five was approached from United Synagogue and Union of Orthodox Hebrew Congregation membership lists, and adult members of the household were invited to participate. Where all members of a household declined to participate (or after at least 3 failures to contact by telephone) the next household on the list was approached.
Each interview took place in the subject's home, and a tape-recording was made whenever the subject was willing. Interviews ranged in length from 1-7 hours, and comprised:
1. The PSE (Present State Examination) (Wing, Cooper & Sartorius, 1973). A shortened form was used, focusing on depression, tension and anxiety symptoms. Symptom level was indicated by the presence of the feature of thought, feeling or behaviour for a duration of at least 2 weeks, at a level which is difficult or impossible to control and which interferes with normal functioning.
2. The LEDS (Life Events and Difficulties Schedule) (Brown & Harris, 1978), slightly modified for use on the target population. The modifications involved the inclusion of questions on: difficulties associated with finding a marriage partner; anti-semitism; involvement with religious cult or missionary groups. Subjects were interviewed about events and difficulties in the 12 months prior to interview, and prior to onset of symptoms where these had been ongoing for more than 12 months.
Completed interviews were written-up and coded using LEDS coding dictionaries and precedents, consensus meetings, and liaison with Tirril Harris and the Medical Research Council team in the Social Policy department at Royal Holloway University of London. A team of seven collaborated on the interviews and coding; all were trained in the use of the LEDS by Tirril Harris. Since all had some knowledge of the main constructs used in this research, interviews were written-up in such a way that coding of events, difficulties and other independent and mediating variables were done independently of the coding of symptoms. Checks on inter-rater reliability showed agreements of 90%, which is similar to the figure of 91% reported by Brown (1989). Measures of stress (see table 2) were based on Brown & Harris's (1978) codings of contextual threat, type of event, focus on the subject and other relevant factors. A stress measure introduced into this study on the basis of observation of the importance of the effects of the recession, was the presence of economic stress (finance, work- and business=related).
3. A demographic and relationships schedule, supplied by Brown & Harris, modified for use on the target population by inclusion of questions on religious observance.
4. Mood and self-esteem measures, not reported further here.
A note on statistical power. The principal analyses were Pearson chi-squares to examine associations in 2 x 2 contingency tables; thus 1 degree of freedom. Assuming a base rate of prevalence of depression of 10%, it was hoped that the investigation would detect differences in rates of depression of 5% for men and 15% for women, against a null hypothesis of 10% in both groups. The index of effect size for chi-square, following Cohen (1992), was calculated to be w=0.23. With a power specification of 0.80, alpha set at 0.05 the sample size required would be N=163. Some unrelated t-tests were carried out; for this, Cohen recommends a minimum N of 64 (where the power specification and alpha as before, and postulating a medium effect size). The size of the samples is thus ample for the principal analyses undertaken on the overall samples. However very small Ns were involved in some analyses, and therefore results of such analyses must be viewed with caution.
RESULTS
1. GENDER DIFFERENCES IN DEPRESSION
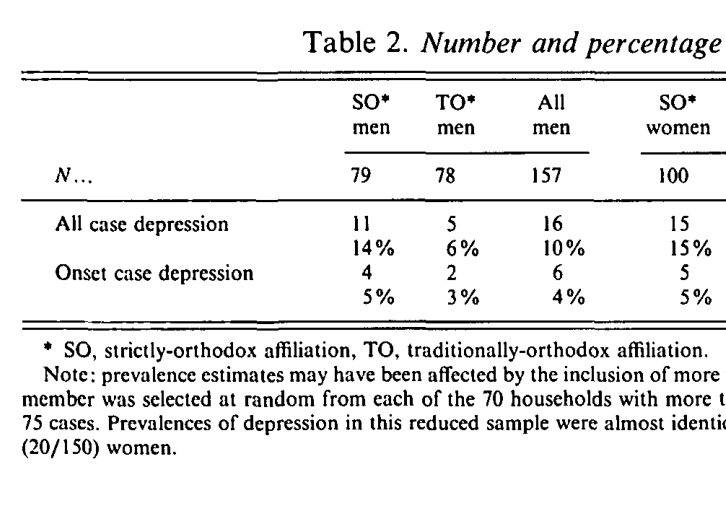
Case depression was defined by the presence of depressed mood plus at least four other symptoms from the 'Bedford College' list (this criterion is very similar to DSM-III major depressive disorder). Table 2 shows the numbers and % of case depression. Two sets of figures are given for case depression. The first set includes 'chronic' cases, where the subject that they had 'always' felt that way, and those with an onset more than 12 months before the date of interview. The second set includes only cases with an onset in the 12 months prior to interview. Borderline states have been excluded from the analyses below.
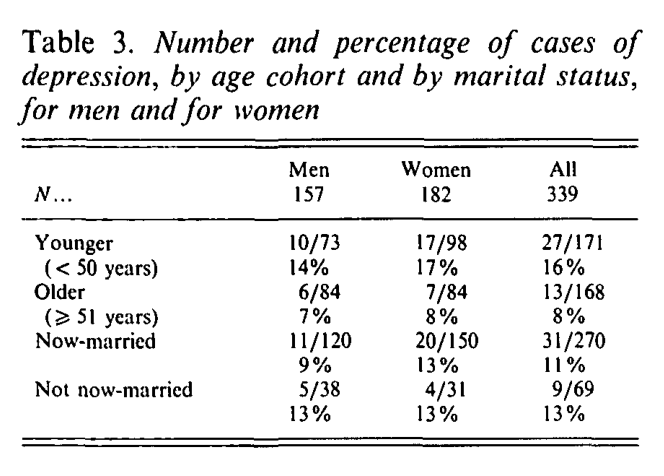
Table 2a breaks down cases of depression by age cohort and by marital status.
Table 2
Table 2a
None of the differences between men and women (or by orthodoxy of affiliation) in Tables 2 and 2a are statistically significant. The largest value of X2 was 2.71 (p=0.1), for the overall effect of affiliation on case depression.
Three possible explanations will be considered.
1. There were no gender differences in social-situational factors and responses to stress.
2. There may be differences in these factors, and these factors may be related to depression, but they worked in opposite directions and effects cancelled each other out.
3. Even if there were gender-related differences in social-situational factors, these factors may not have had the purported effects on depression.
3. GENDER DIFFERENCES IN SOCIAL SITUATION.
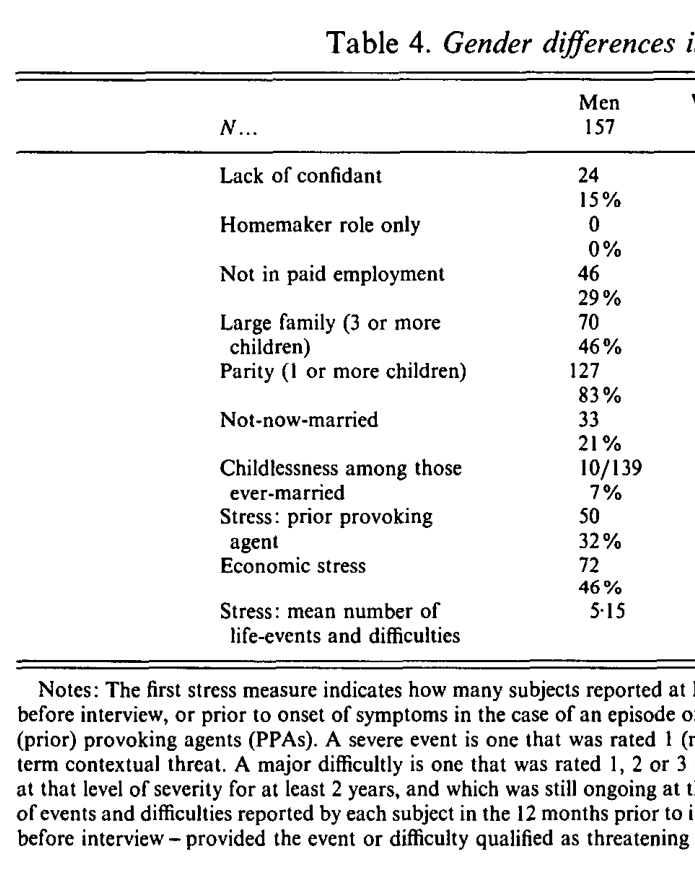
Explanations 1 and 2 may be partly evaluated by examining table 3, which looks for gender differences in social-situational factors (but does not include responses to stress, which appear in table 4).
Table 3
Table 3 shows no gender differences in likelihood of a provoking agent or economic stress, or in marital status, parity and family size (the impact of these factors is conceded to differ for men and for women, however). Women reported more events and difficulties than did men, were significantly more likely not to be in paid employment, to have solely a homemaker role - all these factors have been associated with higher depression in other groups. Women were significantly more likely than men to have at least one confidant - this factor has been shown to be associated with lower depression in other groups.
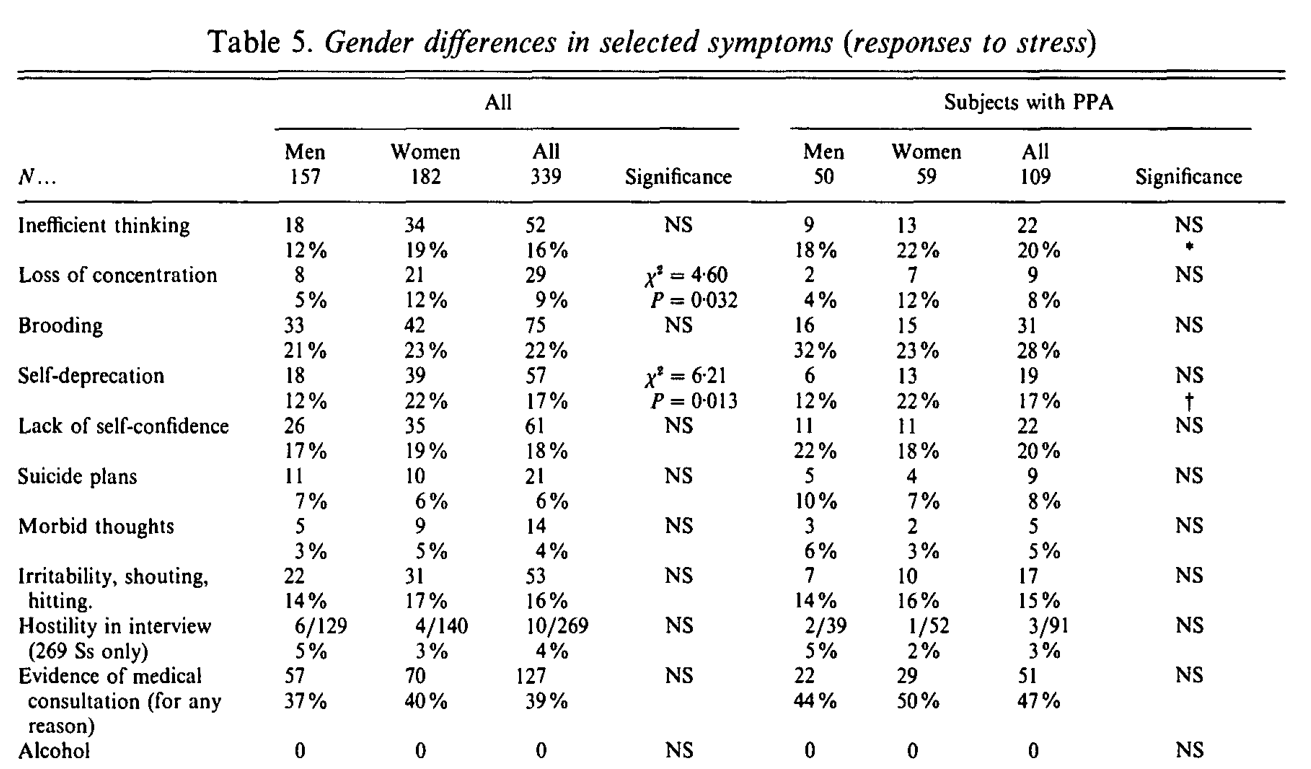
4. GENDER DIFFERENCES IN SELECTED SYMPTOMS (RESPONSES TO STRESS).
Explanations 1 and 2 may also be evaluated by examination of table 4, which looks for gender differences in selected symptoms (responses to stress).
Table 4
Table 4 shows women significantly more likely than men to report loss of concentration and self-deprecation. (Inefficient thinking was also reported more frequently by women than by men, but only in the absence of a provoking agent, so the gender difference of this symptom may not reflect a gender difference in response to stress). The other symptoms examined showed no differences by gender.
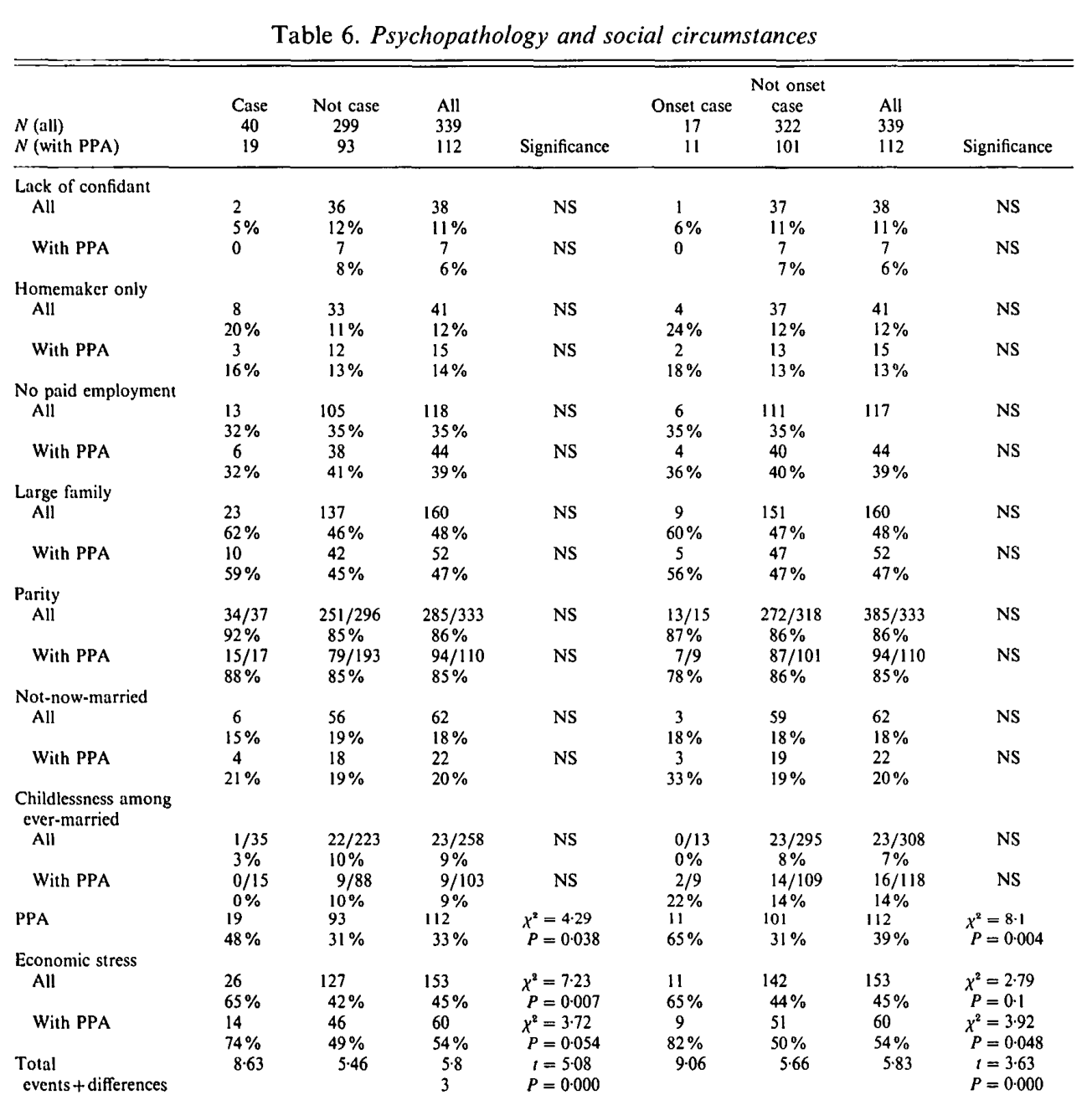
5. ASSOCIATIONS BETWEEN SOCIAL SITUATION AND DEPRESSION
Explanation 3 may be evaluated by examining table 5, which looks for associations between social-situational factors and depression. The associations have been examined among all subjects, and they have also been examined among only those subjects with a prior provoking agent. This second method of analysis follows Brown & Harris (1978), and indicates whether a given factor may act as a vulnerability factor, not causing depression in itself, but making the person more vulnerable to depressive illness in depressing circumstances. The analyses have examined all cases of depression (chronic plus onset), and only those cases with an onset in the previous 12 months.
Table 5
Table 5 shows a clear effect of stress upon depression; this effect is likely to be causal at least where the index of stress is the occurrence of a severe event or major difficulty prior to the onset of depression. Economic stress (work and money-related events and difficulties) appeared as a significant risk factor: the effect was equally marked for men and for women. None of the other factors examined appeared to function as either risk or vulnerability factors.
It was further noted that economic stress was significantly associated with religious affiliation (91/179 - 51% - of the strictly orthodox, compared to 62/160 - 39% - of the traditionally orthodox; X2=5.00, p=.026).
6. CONCLUSIONS
The rates of case depression among the Jewish men and women interviewed did not differ significantly. We have reviewed factors that have been suggested to account for the greater prevalence of female depression in other groups, and examined our data to see whether these factors can account for the similarity in rates of case depression among the men and women interviewed.
Three possibilities were suggested.
The first possibility is that the men and women interviewed did not differ in the presence or absence of the social-situational factors or stress responses examined. There were several such factors and responses in which there were no gender differences:
- there were no differences by gender in likelihood of a provoking agent (severe event or major difficulty), or economic stress - though women's lives were more eventful than the men's;
- there were no gender differences in suicidal plans, morbid thoughts, irritability , hostility or drinking problems (we found no-one reporting a clinical level of alcohol dependency or consumption), or in any symptoms examined other than concentration, inefficient thinking and self-deprecation;
- there were no gender differences in the likelihood of reporting a work or money-related event or difficulty (some other work, such as Kessler & McLeod (1984) has reported that men are more likely than women to report such events);
These similarities between the men and women studied might explain the similarities in the rates of depression. However there were differences by gender in the following respects:
- women were significantly more than likely than men to have at least one confiding relationship;
- the women interviewed were more likely than the men to be engaged solely in a homemaker role;
- women were less likely to be earning.
- although economic stress, marital status, large families and parity were similar among the men and women, those interviewed clearly played different roles in the family, with the women being more occupied with physical and emotional care, and budgeting, while the men were more preoccupied with bringing in enough to support their families. Thus the impact of these factors is suggested to differ for men and for women (as has been suggested for example by Cochrane (1993) for marriage, and by Van Balen & Trimbos-Kemper (1993) for infertility).
- women were more likely to report symptom levels of difficulties with concentration, inefficient thinking and of self-deprecation than men. This is in line with Nolen-Hoeksema's suggestion that women are more likely to ruminate than are men, and Cochrane's suggestion that women suffer from powerlessness.
Since there are several significant gender differences in factors suggested to be related to depression, the second explanation may be considered.
This is that the effects of these gender differences in social circumstances and stress-handling might cancel each other out. However, the differences are generally in the direction that we would expect higher depression among women. The main exception is that women are more likely than men to have at least one confidant. Another possible exception is that few women were in full-time employment, which by comparisons with part-time employment for married women, has been associated with overload. Women and men are equally likely to have suffered a provoking agent; family sizes are similar though women and men clearly played different roles in their families. Women are more likely to be solely occupied with homemaking and not to have paid employment, and they report more numerous threatening events and difficulties. They reported more inefficient thinking, poor concentration and self-deprecation more than did men. In the light of these differences a higher rate of case depression among women than among men might be expected - this however was not the case. Therefore the second possibility does not seem clearly supported.
We now turn to the third possibility, where our evidence suggests that factors which may be associated with depression in other groups may not be associated with depression among those studied here.
Other work on Jewish women (Loewenthal, Goldblatt, Amos & Mullarkey, 1993) suggests that among Jewish women, wellbeing is higher among those whose 'foundation of the home role' is intact. This role is esteemed in Judaism. We might therefore expect lack of earning, caring for a large family and being solely a homemaker may not be associated with depression among women. This was found to be the case. There was an association between family size and depression among men. This may be a function of the responsibility of being the main financial provider for a large family in difficult economic circumstances. The occupational characteristics of the more strictly-orthodox Jews may make them particularly vulnerable to recessionary conditions. Rabbi X is an example:
he has 12 children, and also helps to support his elderly parents. He and his wife are teachers in religious schools. He has not been paid for four months and his wife has not been paid for nearly a year. The bank has been understanding so far, but the X's debts and interest charges are enormous, and the mortgage company is now threatening to foreclose. The Xs have a severely-learning-disabled daughter, and there are constant struggles and heavy financial burdens in giving her the help and care that she needs. Some of the Xs' children are married and have families of their own and Rabbi X feels bad that he cannot help them financially as he would wish to. Rabbi X is also worried about the older unmarried children, for whom good partners must be found.
It was also noted that there was no evidence of alcoholism and little evidence of suicidal intentions - both these escape routes from depression are not normative or generally acceptable among Jews, and their use by men in other groups has been suggested as one explanation for low depression rates among men.
The data also suggest that almost all those suffering from depression have at least one confidant. Confidants are less likely among the non-case-depressed. This suggests that the use of confidants may have been increased - among these subjects - by the depression or by the circumstances leading up to it. It should be remembered that all the subjects were included in the study by virtue of their synagogue membership - this, and the strong family involvements reported by almost all subjects, meant that very few if any subjects were living isolated lives without the possibility of social support should it be needed. Thus the relationship between confidants and depression differed among the Jews studied than amongst the women studied by Brown & Harris, and by others, where lack of a confidant is thought to make for vulnerability to depression. Among those interviewed, it appeared that subjects in depressing circumstances had sought confidants. Brugha & Bebbington's (1990) analyses suggest the helpfulness of this for recovery from depression.
Apart from the stress measures, the social-situational factors which may be associated with depression in other groups, do not function in the same way in the community studied here. Most social-situational factors examined did not appear to be functioning either as risk or as vulnerability factors. It is suggested that the social-situational factors studied may have culture- and cohort-specific effects on depression. Here, for example, there appear to be culture- and possibly cohort-specific relationships of family roles, confiding, and stress-handling, with depression.
The contextual stress measures however did relate to depression. We found in this and other work that these measures adapted readily to use in cultures other than those in which they were originally developed. We would agree with Lora & Fava's (1992) conclusion that the general Brown & Harris (1978, 1989) model relating contextual stress to depression is supported, while the moderating variables vary with culture and cohort.
The rates of depression among the men and women studied were similar. The findings endorse the value of contextual stress measurement for predicting depression, and the findings also endorse previous suggestions that there are gender-, culture- and cohort-specific routes to depression. These routes involve specific cultural-religious values and features. Among the Jews interviewed, the culturally-associated pattern of occupational characteristics, interacting with economic conditions, appeared to have resulted in economic stress which was an important factor contributing to depression among those interviewed. Other important factors were (for women) the esteem attached to the woman's role in family management, and (among Jewish men compared to those in other groups) the low use of alcohol and suicide as escape routes from depression. These culture-specific features appeared to play important roles in affecting the prevalences of depression that were observed.
This research was supported by a project grant from the Economic and Research Council (R000232831). The authors are particularly grateful to Tirril Harris (Medical Research Council Unit, Social Policy Department, Royal Holloway University of London) for her untiring interest and input, to Laurie Letchford for his advice on computing, to Professor Chris Brewin (Psychology Department, Royal Holloway) for his comments on an earlier draft of this paper, to Rosemary Westley (Psychology Department, Royal Holloway), to many rabbis and other communal leaders in the Jewish community for advice, interest and help, and to the subjects who gave their time to be interviewed.
REFERENCES
Ball, R. & Clare, A. (1990) Symptoms and social adjustment in Jewish depressives.British Journal of Psychiatry, 156, 379-383.
Bebbington, P.E., Dean, C., Der, G. & Hurry, J.L. (1991) Gender, parity and the prevalence of minor affective disorder. British Journal of Psychiatry, 158, 40-45.
Bebbington, P., Katz, R., McGuffin, P. & Tennant, C. (1989) The risks of minor depression before age 65: results from a community survey.Psychological Medicine, 19, 393-400.
Beck, A.T. & Steer, R.A. (1987)The Beck Depression Inventory. San Antonio: the Psychological Corporation/ Harcourt Brace Jovanovitch.
Berger, B.D. & Adesso, V.J. (1991) Gender differences in using alcohol to cope with depression. Addictive Behaviours, 16, 315-327.
Brown, G.W. (1989) Life events and measurement. In G.W.Brown & T.O.Harris (editors) Life Events and Illness. London: Unwin Hyman.
Brown, G.W. & Bifulco, A. (1990) Motherhood, employment and the development of depression: A replication of a finding? British Journal of Psychiatry, 156, 169-179.
Brown, G.W. & Harris, T.O. (1978) The Social Origins of Depression. London: Tavistock.
Brown, G.W. & Harris, T.O. (eds) (1989) Life Events and Illness. London: Unwin Hyman.
Brugha, T.S. & Bebbington, P. (1990) Gender, social support and recovery from depressive disorders: A prospective clinical study. Psychological Medicine, 1990, 20, 147-156.
Calloway, P. & Dolan, R. (1989) Endocrine changes and clinical profiles in depression. In G.W.Brown & T.O.Harris (eds) Life Events and Illness. London: Unwin Hyman.
Carta, M.G., Carpiniello, B., Morosni, P.L. & Rudas, N. (1991) Prevalence of mental disorders in Sardinia: a community study in an island mining district. Psychological Medicine, 21, 1061-1071.
Cochrane, R. (1983) The Social Creation of Mental Illness. London: Longman.
Cochrane, R. (1993) Women and depression. In C.A. Niven & D. Carroll (editors) The Health Psychology of Women. Switzerland: Harwood Press.
Cohen, J. (1992) A power primer. Psychological Bulletin, 112, 155-158.
Gater, R.A., Dean, C. & Morris, J. (1989) The contribution of childbearing to the sex difference in first admission rates for affective psychosis. Psychological Medicine, 19, 719-724.
Golding, J.M., Burnam, M.A. & Wells, K.B. (1990) Alcohol use and depressive symptoms among Mexican Americans and non-Hispanic Whites. Alcohol and Alcoholism, 25, 421-432.
Gove, W.R. (1972) The relationship between sex roles, marital status, and mental illness. Social Forces, 51, 34-44.
Harris, T., Surtees, P. & Bancroft, J. (1991) Is sex necessarily a risk factor to depression? British Journal of Psychiatry, 1991, 158, 708-712.
Hobfoll, S.E. (1991) Gender differences in stress reactions: women filling the gaps. Psychology and Health, 5, 95-109.
Hong, S.M. & Grambower, T. (1986) Do women still differ from men? Psychological Reports, 59, 1332.
Ingram, B. & Lowe, D. (1989) Counselling activities and referral practices of Rabbis. Journal of Psychology and Judaism, 13, 133-148.
Jenkins, R. (1985) Sex differences in minor psychiatric morbidity. Psychological Medicine; Monograph Supplements, 7.
Joyce, P.R., Oakley-Brown, M.A., Wells, J.E. & Bushnell, J.A. (1990) Birth cohort trends in major depression: Increasing rates and earlier onset in New Zealand. Journal of Affective Disorders, 18, 83-89.
Kessler, R.C. & McLeod, J.D. (1984) Sex differences in vulnerability to undesirable life events. American Sociological Review, 49, 620-631.
Kosmin, B.A. & Grizzard, N. (1975) Jews in an Inner London Borough - Hackney. London: Board of Deputies of British Jews.
Kosmin, B.A. & Levy, C. (1983) Jewish Identity in an Anglo-Jewish Community. London: Research Unit Board of Deputies of British Jews.
Lehtinen, V., Lindholm, T., Veijola, J. & Veisanen, E. (1990) The prevalence of PSE-CATEGO disorders in a Finnish adult population. Social Psychiatry and Psychiatric Epidemiology, 25, 187-192.
Levin, J.S. (1994) Religion and health: Is there an association, is it valid, and is it causal? Social Science and Medicine, 38, 1475-1482.
Loewenthal, K.M. (1993) Levels of wellbeing and distress in orthodox Jewish men and women. Journal of Psychology and Judaism, 16, 225-233.
Loewenthal, K.M. (1995) Mental Health and Religion. London: Chapman & Hall.
Loewenthal, K.M. & Goldblatt, V. (1993) Family size and depressive symptoms in orthodox Jewish women. Journal of Psychiatric Research, 27, 3-10.
Loewenthal, K., Goldblatt, V., Amos, V. & Mullarkey, S. (1993) Some correlates of distress in Anglo-Jewish women. In L.Brown (ed) Religion, Personality and Mental Health. New York: Springer-Verlag.
Loewenthal, K.M., Gorton, T. & Goldblatt, V. (in preparation) The Usual Mood Checklist.
Lora, A. & Fava, E. (1992) Provoking agents, vulnerability factors and depression in an Italian setting: A replication of Brown and Harris's model. Journal of Affective Disorders, 24, 227-235.
Lowe, C.R. & Garratt, F.N. (1959) Sex pattern of admission to mental hospitals in relation to social circumstances. British Journal of Preventive and Social Medicine, 13, 88-102.
Maton, K.I. (1989) The stress-buffering role of spiritual support: cross-sectional and prospective investigations. Journal for the Scientific Study of Religion, 28, 310-323.
Moeller, T.P., Bachmann, G.A. & Moeller, J. 1993 The combined effects of physical, sexual and emotional abuse during childhood: long-term health consequences for women. Child Abuse and Neglect, 17. 623-640.
Murphy, J.M. & Leighton, A.H. (1989) Repeated investigations of prevalence: the Stirling County study. Acta Psychiatrica Scandinavica, 79, 45-59.
Newman, J.P. (1986) Gender, life strains and depression. Journal of Health and Social Behaviour, 27, 161-178.
Nolen-Hoeksema, S. (1987) Sex differences in unipolar depression: evidence and theory. Psychological Bulletin, 101, 259-282.
Paykel, E.S. (1991) Depression in women.British Journal of Psychiatry, 158, 22-29.
Potts, M.K., Burnam, M. & Wells, K.R. (1991) Gender differences in depression detection: a comparison of clinician diagnosis and standardized assessment. Psychological Assessment, 3, 609-615.
Robbins, C.A. & Martin, S.S. (1993) Gender, styles of deviance and drinking problems. Journal of Health and Social Behaviour, 34, 302-321.
Rorsman, B., Grasbeck, A., Hagnell, O. & Lanke, J. (1990) A prospective study of first-incidence depression: the Lundby study 1957-1972. Special Issue: Cross-Cultural Psychiatry. British Journal of Psychiatry, 156, 336-334.
Rosenfield, S. (1992) The costs of sharing: wives' employment and husbands' mental health. Journal of Health and Social Behaviour, 33, 213-225.
Shmool, M. & Cohen, F. (1990) British Synagogue Membership in
1990. London: Research Unit of the Board of Deputies of British Jews.
Shmool, M. & Miller, S. (1994) Women in the Jewish Community: Survey Report. London: Women in the Community.
Silverstein, B. & Perlick, D. (1991) Gender differences in depression; historical changes. Acta Psychiatrica Scandinavica, 84, 327-331.
Steer, R.A., Beck, A.T. & Brown, G. (1989) Sex differences on the revised Beck Depression Inventory for outpatients with affective disorders. Journal of Personality Assessment, 53, 693-702.
Van Balen, F. & Trimbos-Kemper, T.C.M. (1993) Long-term infertile couples: a study of their well-being. Journal of Psychosomatic Obstetrics and Gynaecology, 14, 53-60.
Vredenburg, K., Krames, L. & Flett, G.L. (1986) Sex differences in the clinical expression of depression. Sex Roles, 14, 37-49.
Waterman, S. & Kosmin, B.A. (1986) British Jewry in the Eighties. London: Research Unit Board of Deputies of British Jews.
West, R. (1991) Computing for psychologists. London: Harwood Academic Publishers.
Wilhelm, K. & Parker, G. (1989) Is sex necessarily a risk factor to depression? Psychological Medicine, 19, 401-413.
Wing, J.K., Cooper, J.E. & Sartorius, N. (1973) The Measurement and Classification of Psychiatric Symptoms. London: Cambridge University Press.
Zuckerman, M. & Lubin, B. (1963) The Multiple Affect Adjective Check List. California: Edits.