Introduction: U.K. Jewry Demography and Psychiatric Epidemiology
There are approximately 13 million Jews worldwide, about 5'/2 million each in Israel and the U.S.A. The remainder are scattered worldwide, with significant
Address for Correspondence: El Kate Miriam Loewenthal, PhD, Psychology TW20 OEX, U.K.^ c.loewenthal@rhuLac,uk
university, Wales, Heythrop College, London University, London, U.K.
concentrations (% to V2 million) in France, Canada, the U.K., Argentina and Russia, and smaller concentrations elsewhere (1). Worldwide, about 80% are said to be Ashkenazim ("Western" Jews), 20% Sephardim, although definitions of these categories are variable. Of approximately 300,000 U.K. Jews, about 10% are estimated to be Sephardic (in the absence of published data, this estimate was offered by the U.K. Sephardic Chief Rabbi, Abraham Levy, in a recent conversation). About -¡3 of U.K. Jews are concentrated in the Greater London area, and most of the remainder in larger provincial cities such as Manchester, Leeds and Birmingham. However, there is wide scattering: there were some Jews in all but one of the 408 U.K. census districts in 2001 (2). About V,i of affiliations are to the orthodox United Synagogue and its provincial affiliates, with the remainder fairly evenly divided between other orthodox groups, particularly the strictly orthodox (haredi) Union of Orthodox Hebrew Congregations, and the Federation and Sephardi groups of synagogues, and the non-orthodox groups (Massorti, Reform, Liberal). In this article, affiliative groups will be referred to as haredi (strictly-orthodox), (traditionally) orthodox, non-orthodox and unaffiliated. Numbers of unaffiliated Jews are hard to estimate, but it has been pointed out that a high proportion of Jews will affiliate in order to secure Jewish burial rites (3). Census data are treated with caution since some Jews were known to be wary of identifying themselves as such, in spite of encouragement to do so (4). While estimates of numbers of Jews are likely to be under-estimates, they may not be major under-estimates. Jews are a small minority (0.5%) among the U.K.'s 62 million, and few compared with the estimated 3 million Muslims in the U.K., who thus outnumber Jews by about 10:1. There is an unusual feature of Anglo-
Department, Royal Holloway, University of London, Egham, Surrey
Jewry, by comparison with virtually all other Jewish communities worldwide, namely that most Jews are affiliated with an orthodox synagogue, even though individual observance is not always strict. This level of orthodox affiliation implies a strong sense of Jewish identity, reflected for example in the relatively low rate of intermarriage: % of married Jews have Jewish spouses (2). In other Diaspora communities, normative affiliation is not with an orthodox congregation, and levels of intermarriage are generally higher. Levels of education and prosperity are at or above U.K. averages (2), for example Jews were more likely than the general population to have a degree-level qualification, to be in full-time employment and to own their own homes. Family size is slightly below the U.K. norm of approximately two children per household. Among the haredim, levels of (secular) education and of prosperity are low, while family size is large (2, 5). Thus in Hackney, the principal haredi area, proportions of Jews with no qualifications, living in rented accommodation, and living in overcrowded conditions, were higher than the national average. What about the psychiatric epidemiology in the U.K. Jewish community? Reliable data are scarce. Several suggestions have been made about psychiatric epidemiology among Jews, and we examine the U.K. evidence: raised prevalence of depressive disorder in Jewish men, low prevalence of alcohol related disorders and suicide, higher prevalences of obsessive-compulsive disorder and psychosis. Anxiety, eating and childhood disorders are also examined in this article.
AIMS and Questions
This article examines mental health and mental health care for Jews in the Diaspora, with a focus on the U.K. How are mental health issues affected by the Diaspora and particularly the U.K. context? The U.K. is the focus since systematic searches for work on Jewish mental health in the Diaspora yield rather fragmentary results. The author has a more detailed knowledge of the situation in the U.K., both fi"om her own research and from work and other experience in the community. Occasional reference will be made to work in other Diaspora countries and Israel, but this article does not aim to make detailed systematic comparisons with Israel, on which a mine of recently-gathered information exists (6).
Depression and Gender
Some years ago I was gazing in alarm at some research results. We had completed a survey of 339 U.K. Jews, involving lengthy life-events interviews and psychiatric assessments. The latter were estimates of caseness based on the Present State Examination (PSE) (7) using criteria similar to DSM-III. We found similar 12-month prevalence of (unipolar) depression among men (10%) and women (13%) (8). Was there something wrong with our data? Most other work reported higher incidence and prevalence of depression among women, compared to men (9, 10): Worldwide, prevalence ranges from 3% to 17%, and 12-month prevalences are about twice as high for women (approximately 10%) as for men (approximately 5%) (9,10). To my relief, other work was emerging that reported similar findings to ours, using DSM-III criteria: Jewish men are as likely as Jewish women to be clinically depressed (11,12), although this is not universally the case (13). Among explanations of this effect are low levels of alcohol use among Jewish men, compared to men from other groups (8, 14, 15). Moderate alcohol use may be an escape route from distress and depression (14, 15). Also, there are reported lower levels of physical violence among Jews than among other groups (16) which may reduce depression among women resulting from domestic violence. A further factor is that Jewish men may be somewhat more willing than men from other groups to talk about symptoms of depression (17).
Alcohol and Substance Abuse
Since the 1950s there has been work on the very moderate use of alcohol among Jews (18) - less than 1% of Jews in the U.S. are alcoholic, compared to 7% in the general population. It was suggested that the vulnerable position of Jews in society leads to an emphasis on self-control. Moreover the encouragement of drinking (and even occasional drunkenness) on prescribed religious occasions limits the use of alcohol. The drift from orthodox affiliation and practice has not been associated with a noteworthy rise in alcohol use or abuse, and it was suggested in 1980 that low use of alcohol among Jews was a persistent community norm (19). This may be exacerbated by genetic factors: a suggested basis is the alcohol dehydrogenase (ADH) enzyme, associated with an aversion to alcohol and a lower risk of alcoholism among Asians and Jews (20). Does low Jewish
alcohol use persist in the U.K.? Low levels of alcohol use among U.K. Jewish men compared to men from other groups were reported in 1990 (14). Recently, a young (male) Jewish student in the U.K. described his bewilderment at the prolific use of alcohol by his nonJewish fellow-students: they seemed to enjoy getting drunk on a daily basis. In a 2003 U.K. study of Jews and Protestants, we noted that the Jews saw drinking and drunkenness as inappropriate for improving mood or socialising (21): "I find that there are better ways to unstress myself, I do not drink when I am low. When I am low, I seek insight. Alcohol does not guarantee insight or even elevated mood" "It's (drinking alcohol/going to the pub) not thefewish way of doing things - you go to a wedding or Bar Mitzvah to meet people" (21). In the U.K., pubs (public houses licensed for the sale and consumption of alcoholic drinks) are a national institution. Jews saw these as wild and violent places. Protestants (except for the more religious) saw pubs as places for socializing and relaxing, where a drink among friends is calming and helps one to forget worries. Jews, women and the more religious reported lower levels of alcohol use than Protestants, men and the less religious (22). Thus religious practice may reinforce culturally carried norms about alcohol use. What about abuse of alcohol? Loewenthal et al.'s (22) sample was composed of strictly and traditionally-orthodox Jews, and there was no evidence of alcohol abuse in this sample. Does psychoactive substance abuse exist among Jews in the U.K.? While there are reports of this, particularly among adolescents, there are no systematic published data. A Chabad house in the London area with a wellestablished drugs helpline reported increased use from Jews (from 85 callers in 2008, to 168 in 2009) (23). This may possibly reflect increased drug use, or increased willingness to seek advice from this source, perhaps due to increased public awareness of the helpline.
SUICIDE While there are tragic instances of suicide among Jews under severe threat, suicide is normally forbidden under Jewish law. Suicide prevalence figures suggest that worldwide, suicide may be lower among Jews, and among other religious groups which prohibit suicide (notably Islam), than among other groups (24-26). In the U.K., fewer suicidal ideas and lower endorsement
of statements tolerant of or favorable to suicide were reported among Jews than among Protestants (27).
Obsessive Compulsive Disorder {OCD) and Other Anxiety Disorders
There is a common suspicion that the detailed requirements of Jewish law may foster OCD. Is this true? Outside the U.K., it has been concluded that religion provides an arena for the expression of OCD among Jews and others (28,29). It has also been shown that obsessional personality traits are associated with religiosity, but not clinical levels of OCD (30). However, there is no direct evidence on links between Jewish religious afliliation or practice, and OCD in the U.K. UK. work reported elsewhere in this article found such negligible levels of OCD caseness that they could not be analyzed (31). What about other forms of anxiety? In the U.K., 12-month prevalence of total anxiety disorders was 6% (31), which is towards the low end of the wide range (4.2%-17.2%), reported in other studies of anxiety prevalence, with 10.6% estimated for 12-month prevalence worldwide (32). In the U.K. study, there were higher levels of borderline clinical anxiety among orthodox (both traditional and haredi) women (38%), compared to men (24%). Afliliation differences were negligible, as were gender and afliliation differences in case anxiety. Why was this? Orthodox women reported higher levels of eventfulness than men, and eventfulness was tied to anxiety. Eventfulness was a product of family size, a feature of haredi life, but the analyses indicated that it was not solely family size that generated anxiety. The traditionally-orthodox women had smaller families than the haredi women, but were as likely to report high levels of eventfulness and of anxiety. It was suggested that "strong obligation and commitment to family and community is as likely in the traditionally as in the strictly-orthodox" (31, 33, 34). Among the specific forms of anxiety, there were significant gender differences only in situational anxiety, again higher among women (25%) than men (13%). It remains to be seen whether these trends in anxiety are specific to the U.K. or apply to Jews elsewhere in the Diaspora. One study (using a symptom checklist) reported low levels of anxiety among Soviet immigrants to the U.S. (35), but outside Israel there is limited other work on anxiety among Jews, and negligible attention on borderline anxiety. Provisionally, prevalence of total
anxiety disorders may be relatively low among UK. and possibly other Diaspora Jews.
PSYCHOSIS Are Jews - Ashkenazi or otherwise - more prone to psychotic illness than other groups? Although this suggestion has been floated in the past, it has recently been contended that there are genetic loci that contribute to susceptibility to schizophrenia, bipolar disorder, and schizoaffective disorders (36), and it is not apparent that Jews are more genetically susceptible than others. There is no evidence from U.K. Jews affecting this point.
Other Disorders: Eating Disorders and Childhood Disorders
Are there other psychiatric disorders that may be more or less prevalent in Jews than in other groups of people. What is the U.K. evidence? There is rising concern about eating disorders, particularly among adolescent girls, with concern expressed by mental health service providers and educators within the U.K. orthodox Jewish community. This brief overview will refer to the most salient eating disorder, anorexia nervosa. It is possible that girls within the haredi community are less subject to media pressure towards slimness than are other girls. Haredim are more isolated from the popular media, TV and internet. Thus haredi girls may be less prone to eating disorders. There is no UK. evidence, though more disordered eating attitudes were reported among Jewish than non-Jewish adolescents in Canada (37). However, this sample included adolescents from across the religious spectrum so we can draw no conclusions about haredi girls. In the U.S. (38), less body dissatisfaction and shame regarding appearance were reported by religious Jewish women, compared to secular Jewish women, suggesting that the insulated rehgious group may protect from body dissatisfaction. This protection may be disappearing, though. The author has noted that U.K. haredi parents believe that overweight daughters will be less marriageable than slim girls, and some haredi young men have confirmed that they would prefer a shidduch (marriage introduction) with a slim girl. Moreover, there is endorsement by educators and community leaders for the encouragement of healthy eating and the avoidance of obesity, for valid health reasons. Thus there are cultural pressures within the haredi community towards dieting and slimness.
But in spite of concern, there is as yet, no reliable U.K. evidence about the prevalence of eating disorders in the haredi or wider Jewish community. Turning to childhood disorders, lower levels of childhood emotional and behavior disturbances were noted in a U.K. pre-school haredi sample (39) compared with other groups assessed using the SDQ. The SDQ (Strengths and Difficulties Questionnaire, a checklist measure) (40) assesses aggressive, anxious, withdrawn, hyperactive and (low) prosocial behavior. However, in another study on older U.K. haredi children and adolescents using the SDQ, teachers reported higher than average levels of hyperactivity and attention disorder among adolescent haredi boys (41). Perhaps the reported problems resulted from the expectation that haredi boys should spend long hours in religious study, with the under-resourced, under-funded schools unable to provide sufficient exercise facilities. Pre-adolescent children, and girls, who are not subject to the same pressures for extensive religious study, and who may have more exercise opportunities as a result of slightly more state funding assistance, were not reported to have raised hyperactivity and attention difficulties. Levels of economic privation among haredim are high, but their disturbing effects may be offset by family cohesion, social support and religious factors. There is scope for more exploration of levels of childhood disorders and their possible causes among Jews. Although it has been suspected that Ashkenazi Jews might be genetically susceptible to autism, as to schizophrenia (42), this is now no longer certain. Childhood disorders - ADHD, autism, learning difficulties and others - need specialist, culturally-sensitive support and treatment, shortly to be discussed.
Lifestyle and Stress in Relation to Psychiatric Disorder
Jewish lifestyle is distinctive, especially among the more religiously-observant. The orthodox will observe the Sabbath, holidays, the dietary and marriage laws, and will prefer their children to have Jewish education. Among the haredim, media exposure is very limited, particularly because of a wish to insulate from differing standards of sexual morality. The practice of charity - giving money and time to communal needs - is heavily valued (5), and more orthodox men attend regular public prayers. Therefore, the religiously-observant - traditional as well as strictly-orthodox - will congregate in areas with
religious amenities available: kosher shops, synagogues, schools, ritual bath-houses. Social hfe with other Jews will be readily available. The strictly orthodox may do little socializing outside their community. Occupations are consistent with religious practice and values, for instance teaching in Jewish schools, or running businesses meeting community needs. Especially for those with large families, finance may be a source of stress, but there is some welfare provision, including child benefit payments. Health care is free under the U.K. National Health Service, and some Jewish schools do now receive state aid. However, many Jewish schools do not, especially in the haredi sector, and the provision of Jewish education is a drain on parental and community resources (5, 8). All the above has mental health implications. The main positive features of Jewish lifestyle include the benefits of religiosity, including protective religious beliefs, prayer, social support, and family stability. There are negative mental health implications, but these overall would normally be outweighed by the benefits. Negative aspects include the impact of family size when income is inadequate, the complex effects of low alcohol use, and the closed community. Tlie closed community can result in the need to maintain reputations, thus fear of betraying imperfection and avoidance of help-seeking for mental health problems, sometimes resulting in a downward spiralling into a more severe mental illness. Firstly, religiosity has been found in other culturalreligious communities, and in Jews in the U.K. and elsewhere, to be associated with better mental health (43-45). Underlying this overall effect are the benefits of trust in G-d, hope, prayer, spiritual support, and other positive coping beliefs (46). Some of these effects have been confirmed in the U.K. Jewish community (47). Social support and family cohesiveness are also beneficial (41). Social support includes neighborly help from other community members, and specific culturallysensitive community services (48, 49). Unlike in the wider (non-Jewish) community, family size - religiously encouraged among haredim - does not in itself make women or men vulnerable to depressive disorder (8). Indeed it has been reported that women with large families report some mental health benefits, for example better concentration, compared to Jewish women with smaller families (50). But financial hardship can impact negatively on mental health, especially when family size is large. In the U.K., men seem more vulnerable to this effect than women (8). And as described earlier, family size is associated with eventfulness, which is associated
with borderline case anxiety particularly among women (33). Family stability - as indicated by the relative rarity of family conflict, violence and divorce - is associated with low levels of case depression (34). As described, cultural norms mean that alcohol is not normally used for coping, and this may be a cause of raised levels of depression among Jewish men (15). The closed community entails effort of reputation-maintenance, which may impact on seeking help for mental health problems. Another facet of reputation-maintenance is the silence which surrounds child and domestic abuse. There is reluctance (on religious grounds) to report instances to the civil authorities, and unwillingness to believe that respected members of the community may have perpetrated abuse. These phenomena have received limited attention, except among professionals working within the community. There is some suggestion that physical and sexual abuse may be lower among Jews than other in other groups (16), but information is limited: systematic data may be hard to obtain, though as mentioned lower levels of family conflict were reported among the Jewish community in the U.K. (34). This section looked at some lifestyle factors and their possible impact upon mental health. Effects are mixed, but possibly beneficial overall. There is certainly scope for a closer look at these effects.
Service Provision
Mental health service provision is dominated by the National Health Service. In spite of imperfections and funding cuts, it still offers a generally high quality of health care to U.K. citizens free of charge. Mental health services are provided under the National Health Service via general practitioner (GP) (family medicine) surgeries, including medication, counselling, and referral to specialist psychiatric hospitals with in-patient and outpatient facilities. For minority groups there may be failures to meet cultural needs (51). Examples include professional misinterpretation of religious behavior, such as religiously-prescribed handwashing, as obsessional (52), and difficulties experienced by Jewish parents in getting culturally appropriate provision for children with special needs (49). Numerous Jewish charitable bodies have arisen, designed to meet the needs of the Jewish community. These range from the relative giants, Jewish Care and Norwood/Ravenswood, which cover the spectrum of mental health, special-educational and social service needs for the whole community, to a host of relatively small haredi organizations such as Chizuk,
MENTAL HEALTH AND MENTAL HEALTH CARE EOR JEWS IN
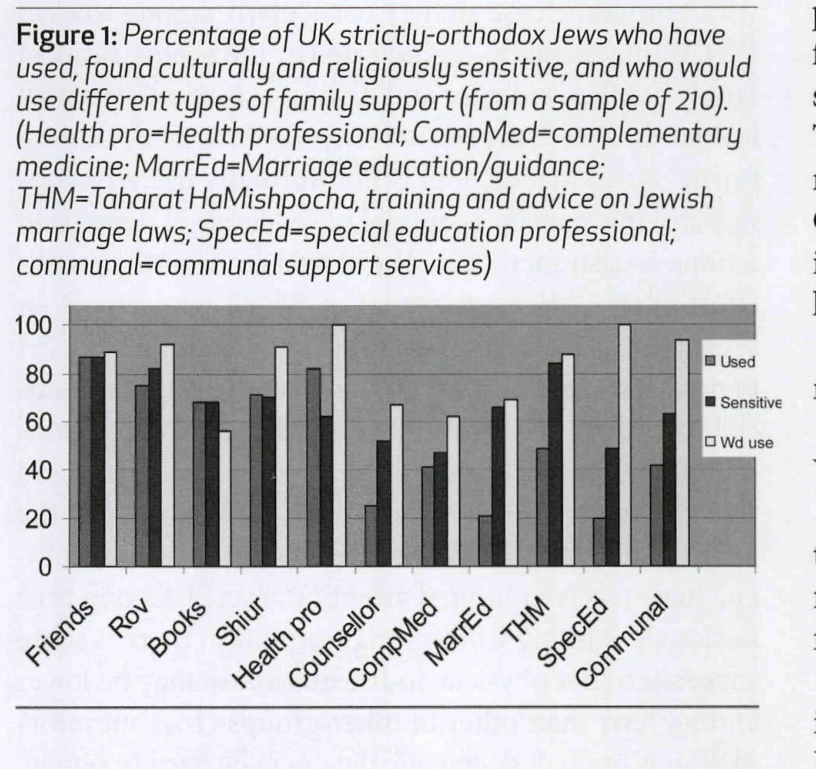
Figure 1: Percentage af UK strictly-orthodox Jews who have used, found culturally and religiously sensitive, and who would use different types of family support (from a sample af210). (Health pra=Health professional; CampMed=camplementary medicine; MarrEd=Marriage educatian/guidance; THM=Taharat HaMishpocha, training and advice an Jewish marriage laws; 5pecEd=special education professiona/; communol=communo/ support services]
offering psychiatric support and preventive work, and Ezer LeYoldos, offering support and counselling for mothers of newborns (48). Rabbis and their wives offer considerable support and counselling (49, 53). In the private sector, there is a growing army of orthodoxJewish counsellors and psychotherapists. To what extent are these different services used or avoided, and why? Figure 1 offers some comparison of the use, perceived cultural sensitivity, and willingness to use, for different services for family difficulties, as reported by 230 U.K. strictly-orthodox Jews (49). The sample comprised those who responded to a postal survey addressed to 1,500 households randomly selected from Union of Orthodox Hebrew (strictly-orthodox) congregation membership lists. The 14% response rate was considered satisfactory for a postal survey. The average number of children per household was 5.6, similar to that reported in other studies of strictly-orthodox Jews, supporting the possibility that the sample may be representative of strictly-orthodox Jews in the U.K. Unfortunately, there are no comparable data for other U.K. Jews. The commonly-used forms of support are generally those regarded as socially acceptable and which carry little or no stigma. For psychological difficulties, there is an over-riding need to maintain personal and family reputation, as in other cohesive cultural-religious groups (54, 55). The stigma of mental illness may affect marriageability for the whole family. Attending a GP surgery is non-stigmatizing and is a popular option (49). Similarly, consulting a rabbi is also a
popular option. Visits to psychiatric clinics are made furtively and reluctantly, with fear of being misunderstood by non-Jewish or non-religious professionals. Therefore, many personal and spiritual difficulties may not be addressed, unhelpful for therapeutic progress. Culturally-sensitive services within the community involve a different set of problems - the risk that problems may become public knowledge (56). "I would not see a counsellor in the community. I might find myself sitting next to her at a wedding." "I wouldn't go to a support group in the community. We live in a goldfish bowl." (48) Further, there are fears that haredi and other Jewish therapists and support workers are somehow less "professional," less well-trained and less discreet than professionals from the general community (48). Solutions to these dilemmas include the training in cultural needs of professionals within the National Health Service, and in the educational support and social services. Private and voluntary sector service providers must be above reproach with regard to confidentiality and professionalism. Services for child and other domestic abuse need development.
Comparison with Other Diaspora Communities
How does the situation in the U.K. compare with that in other Diaspora countries? Lack of studies using comparable research questions and methods make confident comparisons and conclusions difficult. There are some possible suggestions. First, where comparable information exists, psychiatric epidemiology among U.K. and other Diaspora Jews may have broadly the same features. Thus depression may be more common among Jewish men than among men from other groups, while anxiety, alcohol and substance abuse may be less prevalent. We cannot draw conclusions about psychosis or childhood disorders. Secondly, the provision of culturally-sensitive services is developing well in all or most Diaspora countries with significant Jewish communities. In particular, the development of psychotherapy appropriate to Jewishis progressing, possibly with diminishing stigma attached to seeking psychotherapeutic help. Childhood disorders present particular problems and often require costly solutions. This situation has a familiar flavor worldwide. Some Diaspora communities have hospital psychiatric service provision designed for the Jewish community. In Europe, there
is now just one Jewish psychiatric hospital, the Sinai Centre in Amsterdam (57). Originally set up to provide support for Holocaust survivors, it now also provides support for non-Jewish survivors of war and genocide. There are several Jewish centers for hospital treatment in the U.S., in which there are psychiatric facilities, for example the Barnes-Jewish hospital (58), staffed by Washington University doctors. The majority of Jews in the Diaspora who require hospital care for psychiatric disorders will not have a specifically Jewish facility available. It is not known how the provision of Jewish hospital facilities affects uptake, but the picture may be extrapolated from the situation in the U.K. Difficulties experienced in general psychiatric hospitals include the fear of cultural and religious misunderstanding, and lack of religious facilities. These barriers are overcome when culturally and religiously-sensitive services are provided. However, the uptake of Jewish services increases the fear of stigmatization (48). Of concern for mental health is the reported rise in anti-Semitism in the U.K., elsewhere in Europe, and worldwide (59). Much of this is thrust forward by Arab anti-Israel sentiment. It was noted that approximately 21% of the social service needs and difficulties reported by Jews were culturally-tinged, specifically Jewish, includSemitism (60). Anti-Semitic incidents include epithets such as "dirty Jews," "send them to the gas ovens (sic)," losing employment because of the need to be Sabbathobservant, and attacks by Muslims and others on Jews, which can have mental health consequences.
CONCLUSIONS Men may be as prone to depressive disorder as women, a tendency which has been noted in some other studies of Jews. Anxiety prevalence, alcohol abuse and possibly suicide are low by world standards. There are few U.K. data on the prevalence of the less common psychiatric disorders - such as psychosis and OCD - among Jews. There is scope for more research on a range of issues, including eating and childhood disorders. Jewish lifestyle may protect from some difficulties, but gives rise to needs for special service provision. U.K. and other Diaspora Jews are vulnerable to mental health difficulties arising from cultural insensitivity and abuse. Protective factors include family stability, social support and religion.
References
1. Jewish population in the world and in Israel. Division of Jewish Demography and Statistics, The A. Harman Institute of Contemporary shnaton61/st02_27.pdf (accessed 23.06.2011). 2. Graham D, Schmool M, Waterman S. Jews in Britain: A snapshot from the 2001 census. London: Institute of Jewish Policy Research, 23.06.2011) 3. Waterman S, Kosmin BA. British Jewry in the eighties. London: Research Unit Board of Deputies of British Jews, 1986. boardofdeputies.org.uk/page.php/Census2011/397/1/13 (accessed 23.06.2011) 5. Holman C, Holman N. Torah, worship and acts of loving kindness: Baseline indicators for the Charedi community in Stamford Hill. Leicester: De Montfort University, 2002. 6. Levav I, editor. Psychiatric and behavioural disorders in Israel. Jerusalem: Gefen, 2009. 7. Wing JK, Cooper, JE, Sartorius N. The measurement and classification of psychiatric symptoms. London: Cambridge University, 1973. 8. Loewenthal KM, Goldblatt V, Gorton T, Lubitsch G, Bicknell H, Fellowes D, Sowden A. Gender and depression in Anglo-Jewry. Psychol Med 1995; 25:1051-1063. 9. Andrade L, Caraveo A. Epidemiology of major depressive episodes: Results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int J Methods Psychiat Res 2003;12:3-2I. 10. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IVdisorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62:617-627. 11. Levav I, Kohn R, Dohrenwend BP, Shrout PE, Skodol AE, Schwartz S, Link BG, Naveh G. An epidemiological study of mental disorders in a 10-year cohort of young adults in Israel. Psychol Med 1993;23: 691-707. 12. Levav I, Kohn R, Golding JM, Weissman MM. Vulnerability of Jews to affective disorders. Am J Psychiatry 1997; 154:941-947. 13. Levav I, Levinson D. The epidemiology of affective disorders in Israel. In Levav I, editor. Psychiatric and behavioural disorders in Israel. Jerusalem: Gefen, 2009:186-199. 14. Ball R, Clare, A. Symptoms and social adjustment in Jewish depressives. Br J Psychiatry 1990;156: 379-383. 15. Loewenthal KM. The alcohol-depression hypothesis: Gender and the prevalence of depression among Jews. In Sher L, editor. Comorbidity of depression and alcohol use disorders. Hauppage, N.Y.: Nova Science Publishers, 2009:31-40. 16. Moeller TP, Bachmann GA, Moeller J. The combined effects of physical, sexual and emotional abuse during childhood: Long-term health consequences for women. Ch Abuse Neglect 1993; 17:623-640. 17. Loewenthal KM, MacLeod AK, Cook S, Lee MJ, Goldblatt V. Tolerance for depression: Are there cultural and gender differences? J Psychiatr Ment Health Nurs 2002; 9:681-688. 18. Snyder CR. Alcohol and the Jews: A cultural study of drinking and sobriety New York, N.Y.: Free Press, 1958. 19. Glassner G, Berg, B. How Jews avoid alcohol problems. Am Soc Rev 1980; 45: 647-664. 20. Neumark YD, Friedlander Y, Durst R, et al. Alcohol dehydrogenase polymorphisms influence alcohol ehmination rates in a male Jewish population. Alcoholism Clin Exp Res 2004; 28: 10-14. 21. Loewenthal KM, MacLeod AK, Cook S, Lee MJ, Goldblatt V. Drowning your sorrows? Attitudes towards alcohol in UK Jews and Protestants: A thematic analysis. Int J Soc Psychiatry 2003; 49: 204-215. 22. Loewenthal KM, MacLeod AK, Cook S, Lee MJ, Goldblatt V. Beliefs about alcohol among UK Jews and Protestants: Do they fit the
MENTAL HEALTH AND MENTAL HEALTH CARE FOR JEWS IN
alcohol-depression hypothesis? Soc Psychiatry Psychiatr Epidemiol 2003; 38:122-127. 23. Martin J. Cans to drugsline double. Jewish Chronicle, Feb 18, 2010. 24. Bertolote JM, Fleischman, A. A global perspective in the epidemiology of suicide. Suicidology 2002;7:6-8. 25. Kohn R, Levav I, Chang B, Halperin B, Zadka P. Epidemiology of youth suicide in Israel. J Am Acad Child Adolesc Psychiatry 1997; 79:468-473. 26. Band M, Dein S, Loewenthal KM. Religiosity, coping and suicidality within the religious Zionist community of Israel. A thematic qualitative analysis. Mental Health Rel Cult 2011 (in press). 27. Loewenthal KM, MacLeod AK, Cook S, Lee MJ, Goldblatt V. Ihe suicide beliefs of Jews and Protestants in the UK: How do they differ? Isr J Psychiatry Relat Sei 2003; 40:174-181. 28. Greenberg D, Witztum E. Sanity and sanctity: Mental health work among the ultra-orthodox in Jerusalem. New Haven and London: Yale University, 2001. 29. Al-Solaim L, Loewenthal KM. Religion and obsessive-compulsive disorder (OCD) among young Muslim women in Saudi Arabia. Mental Health Rel Cult 2011; 14: 169-182. 30. Lewis CA. Cleanliness is next to Godliness: Religiosity and obsessiveness. J Rel Health 1998; 37:49-61. 3 i. Loewenthal KM, Goldblatt V, Gorton T, Lubitsch G, Bicknell H, Fellowes D, Sowden A. The social circumstances of anxiety among Anglo-Jews. J AffDisord 1997; 46: 87-94. 32. Somers JM, Goldner EM, Waraich P, Hsu L. Prevalence and incidence studies of anxiety disorders: A systematic review of the literature. Can J Psychiatry 2006;51: 100-113. 33. Loewenthal KM, Goldblatt V, Lubitsh G.. Haredi women, Haredi man, stress and distress. Isr J Psychiatry Relat Sei 1998; 35: 217-226. 34. Loewenthal KM, Goldblatt V, Lubitsch G, Gorton T, Bicknell H, Fellowes D, Sowden A. The costs and benefits of boundary maintenance: Stress, religion and culture among Jews in Britain. Soc Psychiatry Psychiatr Epidemiol 1997; 32: 200-207. 35. Hoffmann C, Bentson H, McFarland J, Kinzie D, Bresler L, Rakhlin D, Wolf S, Kovas AE. Psychological distress among recent Russian immigrants in the United States. Int J Soc Psychiatry 2006; 52: 29-40. 36. Craddock N, O'DonovanMC, Owen M J. Genes for schizophrenia and bipolar disorder? Implications for psychiatric nosology. Schiz Bull 2006;32:9-16. 37. Pinhas L, Heinmaa M, Bryden P, Bradley S, Toner B. Disordered eating in Jewish adolescent girls. Can J Psychiatry 2008; 53: 601-608. 38. Gluck ME, Geliebter A. Racial/ethnic differences in body image and eating behaviors. Eating Behaviors 2002;3:143-151. 39. Lindsey C, Frosh S, Loewenthal KM, Spitzer E. Emotional and behaviour disorders among strictly-orthodox Jewish pre-school children. Clin Child Psychol Psychiatry 2003; 8: 459-472. 40. Goodman R. The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. J Chñd Psychol Psychiatry 1999; 40: 791-801. 41. Frosh S, Lindsey C, Loewenthal KM, Spitzer E. Prevalence of emotional
and behavioural disorders among strictly orthodox Jevrish children in London. Clin Child Psychol Psychiatry 2005;10:351-368. 42. Goodman A. A family history study of schizophrenia spectrum disorders suggests new candidate genes in schizophrenia and autism. Psychiatr Q 1994; 65:287-297. 43. Koenig HB, McCullough ME, Larson DB. Handbook of religion and health. Oxford: Oxford University, 2001. 44. Rosmarin DH, PargamentKI, MahoneyA. The role of religiousness in anxiety, depression, and happiness in a Jewish community sample: A preliminary investigation. Mental Health Rel Cult 2009;12:97-113. 45. Rosmarin DH, Krumrei EJ, Andersson G. Religion as a predictor of psychological distress in two religious communities. Cog Behav Therapy 2009; 38:54-64. 46. Pargament K. The psychology of religion and coping. New York: Guilford, 1997. 47. Loewenthal KM, MacLeod AK, Goldblatt V, Lubitsh G, Valentine JD. Comfort and joy: Religion, cognition and mood in individuals under stress. Cog Emotion 2000;14: 355-374. 48. Loewenthal KM, Rogers MB. Culture sensitive support groups: How are they perceived and how do they work? Int J Soc Psychiat 2004; 50; 49. Blumenfeld J, Loewenthal KM, Spitzer E. A study of family services use and of service development needs among strictly orthodox Jews in the U.K. Report to the Department for Education and Sciences for Chizuk. London; Chizuk, 2006. 50. Loewenthal KM, Goldblatt V. Family size and depressive symptoms in orthodox Jewish women. J Psychiatr Res 1993; 27:3-10. 51. Bhui K, Olajide D. Mental health service provision for a multi-cultural society. London: Saunders, 1999. 52. Yossifova M, Loewenthal KM. Religion and the judgement of obsessionality. Mental Health Rel Cult 1999; 2: 145-152. 53. Leavey G, Loewenthal KM, King M. Challenges to sanctuary: The clergy as a resource for mental health care in the community. Soc Sei Med 2007; 65; 548-559. 54. Loewenthal KM, Cinnirella M. Beliefs about the efficacy of religious, medical and psychotherapeutic interventions for depression and schizophrenia among different cultural-religious groups in Great Britain. Transcult Psychiatry 1999; 36; 491-504. 55. Cinnirella M, Loewenthal KM. Rehgious and ethnic group influences on beliefs about mental illness: A qualitative interview study. Br J Med Psychol 1999; 72: 505-524. 56. Loewenthal KM. Strictly orthodox Jews and their relations with psychiatry and psychotherapy. Transcult Psychiat Section World Psychiat Assoc Newsletter 2005; 23; 20-24. 57. Skiai Centrum. http;// (accessed 23.9.11) (Dutch) 58. Barnes Jewish Hospital. http;// (accessed 25.9.11) 59. Chesler P. The new anti-semitism; The current crisis and what we must do about it. San Francisco, Cal.: Jossey-Bass. 2003. 60. Loewenthal KM, Goldblatt V, Gorton T, Lubitsch G, Bicknell H, Fellowes D. Welfare needs in the orthodox Jewish community. Report to Jewish Care, 1994.