An analysis of past research obtained through a systematic review suggested that it is possible to explore the relationship between religious identity, level of practice and mental health, especially self-esteem, in religious and non-religious individuals. The results of this interaction are often contradictory in nature. Several theoretical approaches and models were used to illustrate relationships between variables identified through a separate qualitative study (religious identity, religiosity, shame, guilt, forgiveness and self-esteem). The combination of studies on different social, racial, ethnic and religious groups suggest that the contradictory findings might be explained by the possibility that religious identity and different forms of religious practice affect levels of mental health in a unique manner for each social group.
How do religious identity and levels of religious practice influence mental health? This review will provide a brief overview of the conflicting findings in the study of religious identity, level of practice and mental health, address several theoretical and methodological concerns and suggest possible ways of overcoming these concerns in order to further explore the connection between an individual’s religious identity and various aspects of mental health. Suggestions for further research will be addressed. An increasing volume of research has reported contradictory and inconclusive findings in the area of religious identity, religiosity and mental health (e.g. Argyle & Beit-Hallahmi, 1997; Batson, Schoenrade & Ventis, 1993; Brown, 1994; O’Connor, 1998). There is evidence for both the positive and negative effects that religious group membership and level of practice have on physical and mental health (Blaine & Crocker, 1995; Jacobson, 1997; Loewenthal et al., 1997; Luyten, Corveleyn & Fontaine, 1998). O’Connor
(1998) suggests that these research studies have reported ‘discrepant, contradictory, inconsistent and inconclusive findings’ (p.128) because of a number of theoretical and methodological concerns.
Religion and mental health: A brief empirical history Is it possible to explore the connection between an individual’s religion and various aspects of mental health? Questions concerning the effect of religion on mental health were often addressed by the founding fathers of psychology and psychiatry. The publications and debates of James, Freud, Jung and Erickson (among others) are peppered with arguments concerning the origins, functions and outcomes of religious beliefs and religious group membership. Freud and Jung both seemed to agree that, while religion served a function, it arose out of human need often based on delusion. However, Freud viewed the outcome of that function as a negative component of mental health while Jung saw it as a necessary, healthy delusion (Wulff, 1997). By the 1960s, empirical work still led to disagreements concerning the effect of religious group membership (identity) on mental health. After reviewing the studies examining the relationship, James Dittes (1969) concluded that religion is often associated with deficiencies of personality, with a ‘weak’ or ‘constricted’ ego. On the other hand, Becker (1971) concluded that the relationship between religion and mental health is positive by citing correlations between the absence of mental illness and religious identity and activity. Accordingly, Sanua (1969) declined to draw any clear conclusion after his review of the available empirical research (Batson et al., 1993).
Current research More recently, several studies have readdressed the complex relationships between religious identity and mental health, providing support for both the positive and negative effects that religious identity and levels of religious practice have on mental health (Blaine & Crocker, 1995; Jacobson, 1997; Loewenthal et al., 1997; Luyten et al., 1998). These studies will be explored in greater detail throughout the review. While it is evident that religious identity influences levels of mental health in a variety of ways, none of the data has fully demonstrated exactly why and how these interactions exist. Various explanations have been offered for the apparent effects that religious group membership has on mental health. Luyten et al. (1998) summarised the work of Hood, Spilka, Hunberger and Gorsuch (1996) nicely by stating: ‘With empirical evidence, that, depending upon the concrete situation, religion may be an expression of mental illness, may be a socialising and suppressing agent, may serve as a haven from stress, may be therapeutic, or may even be a source of stress’ (p.166). These contrasting functions and outcomes can be seen in the interplay of empirical findings. For example, does the added focus on religious practices enable individuals to deal with ambiguities and contradictions found in their social environment (Jacobson, 1997) or does it increase the levels of stress and tension associated with higher levels of boundary maintenance found in more orthodox individuals (Loewenthal et al., 1997)? Alternatively, does a religious identity generate increased feelings of value and uniqueness, thus allowing religiousness
to act as an adaptive psychological function or coping mechanism (Ganzevoort, 1998) for all religious groups or are the effects more positive for one group, and negative or ineffective for another (Blaine & Crocker, 1995)? Furthermore, do religious beliefs increase levels of shame and guilt or create a buffering effect caused by increased levels of self-esteem that are synonymous with a positive identity (Blaine & Crocker, 1995; Loewenthal et al., 1997)? The full effect of religious identity and level of practice on mental health cannot be uncovered until several methodological concerns are addressed. This review is concerned with gaining a better understanding of the perceived relationship and underlying interactions existing between religious identity, religiosity and mental health. Additionally, it will attempt to highlight the methodological problems associated with studying this relationship in the hope of developing methodology that can be used to move one step closer to addressing the issues surrounding the psychology of religion.
Definitions of religious terminology and mental health Is it possible to establish an all-inclusive definition of religion, identity or mental health? In order to uncover the methodological problems that influence such mixed results in the study of the psychology of religion, it is important to understand the terminology. The areas of religious identity and mental health are extensive fields in which multiple defini-
1 The interview study consisted of 24 interviews, ranging practising Christian (N=13), Muslim (N=5) and employing a combination of grounded theory (Pidgeon, interpretative phenomenological analysis (IPA) (Smith, common themes between the three groups. Based on 13 scores (assessed by the intraclass correlation coefficient)
tions and theories interact. Idler (1995) claimed that, ‘Neither religion nor health is itself a single strand. Religious involvement can mean a mix of practices, beliefs, and identities; health is an even more global concept combining mental, physical, and even social wellbeing’ (p.684). Clearly, it is vital to define these issues by the cultural context in which they are analysed; yet researchers are often forced to rely on broad definitions when discussing the effects of religious group identity on mental health across several different groups. Respondents taking part in a multi-faith qualitative study1 related to this review were asked to generate their own, personal definitions of six common variables (identity, religiosity, shame, guilt, forgiveness and self-esteem). In the interest of space and clarity, generic definitions will be utilised until further clarification can be offered in a future qualitative review. For the purpose of this review, religion will be defined as, ‘The experiences, cognitions, and actions seen (by the individual or community) as significant in relation to the sacred’ (Ganzevoort, 1998, p.260). Religion can also be defined by its function or the system of beliefs and practices by means of which a group of people struggle with the ultimate problems in life (existential questions) (Batson et al., 1993). In turn, identity will function as, ‘The individual characteristics by which a person or thing is recognised’ (Treffry & Ferguson, 2002, p.397). This definition is useful
from 60–120 minutes each) conducted with non-practising (N=6) populations. A thematic analysis 1996), Toulmin’s argumatics (1958) and Jarman & Osborn, 1999) was used to identify randomly-selected interviews, inter-rater reliability fell within the range of accepted levels.
because it incorporates both private and public identities in its simplicity. Religious identity will be understood as the religious group to which an individual belongs or the belief system to which an individual adheres. Further aspects of identity and identity theory will be discussed later in this review. Due to the fact that mental health is an extremely general term, participants taking part in the interview study conducted alongside this systematic review identified self-esteem as a key issue in their day-to-day understanding of the influence of religious identity and religiosity on levels of mental health. Therefore, for the purpose of this review, mental health will be discussed in terms of self-esteem, which is understood as ‘the worth or dignity that one ascribes to oneself’ (Jacoby, 1997, p.24). Mental health will also be understood in terms of the seven distinct conceptions of mental health proposed by Batson et al. (1993). These seven conceptions of mental health were based on a review of over 100 articles analysing the relationship between religion and mental health. Table 1 presents the seven conceptions of mental health proposed by Batson et al. (1993). It should be noted that an individual does not need to possess all of these in order to be viewed as mentally healthy.
1. Lack of mental illness. 2. Pro-social behaviour. 3. Freedom from worry and guilt. 4. Feeling of personal competence 5. Self-esteem, self-acceptance or 6. Organised and unified personality 7. Open mind to new ideas and
The apparent simplicity of these definitions becomes more complicated, however, by the fact that an individual can have multiple identities at any given point in time. It is not difficult to locate an individual who claims to be an active Muslim, Jew or Christian but these identities take on new meaning when coupled with male or female; Black, White, or Asian; rich or poor; young or old; able-bodied or disabled, etc. This review will concern itself only with the definitions of samples found in multiple database searches centred around one question: Is it possible to establish a connection between an individual’s religious identity, level of practice and mental health, in particular, self-esteem?
METHODOLOGY Topics and themes were generated during the previously mentioned multi-faith interview study exploring individual understanding of religious identity, religiosity and mental health.
Search strategy The search strategy was based on the guidelines found in the University of York National Health Service Centre for Reviews and Dissemination (1996). These guidelines propose search strategies for completing systematic reviews of research literature in order to estimate the overall effectiveness of past research
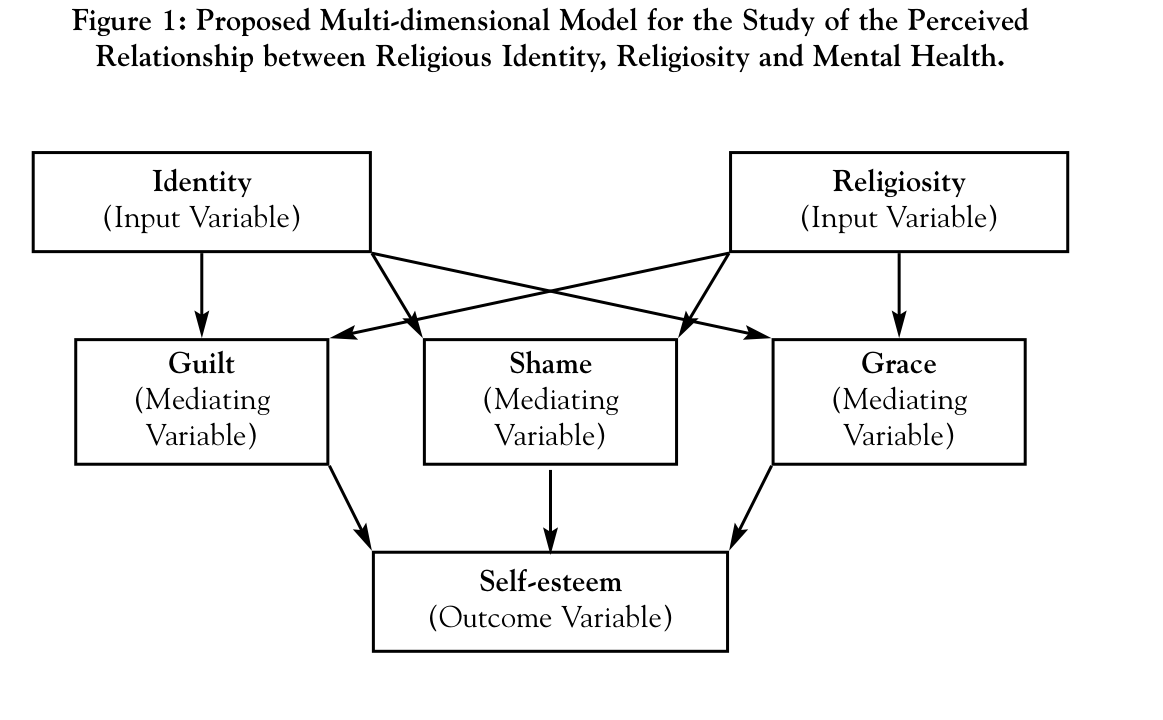
and describe and investigate differences (Treffrey & Ferguson, 2002, p.354). found between previous studies, thus Grace, represents benevolence or, in providing the fullest possible evidence to functional terms, the interpersonal drive informed decision making (NHS process of forgiveness. In future figures, Centre, 1996). The guidelines proposing grace will be labelled as forgiveness. a structure for search terms and search Forgiveness functions on both a cognistrategy were followed after developing a tive and a social level. Forgiveness is multidimensional model for six common defined as ‘The process of letting go of components of religion and mental negative thoughts, feelings, and reactions health identified by the interview study. toward the offender (and often toward Themes common to the practising oneself)’ (Worthington, 1998, p.164). Christians (PC), Muslim (M) and non- It quickly becomes apparent that practising (NP) participants produced these simple, precise definitions fail to the six headings seen in Figure 1. separate the complex components of Within this model, identity refers to shame and guilt. Although both shame the faith system or the religious group to and guilt are negative emotions, it is which each person belongs; religiosity, or important to distinguish between the two religious practice, refers to the way in due to their different implications for which the participants express their interpersonal and intrapersonal funcbeliefs (e.g. prayer, confession, atten- tioning (Tangney, 1995; Tangney, dance), shame is understood as emotions Burggraf, & Wagner, 1995). Qualitative caused by awareness of guilt or dishonour and quantitative studies have illustrated in personal conduct or state (Makins, that guilt is the healthier component, Adams & Knight, 1997). Guilt is defined whereas shame is seen as maladaptive as, ‘The fact, state of having done wrong’ (Luyten et al., 1998). Further similarities
and differences between guilt and shame will be discussed later in this review.
Systematic review Three sets of search terms were used with appropriate symbols in order to assure the words were found in every possible format (e.g. Religi*; Identi*; Self-Accept*; Selfesteem, and self esteem). For example, the first search (Search 1) simply looked at two key words related to religious identity. The second search (Search 2) investigated identity-related processes identified during the qualitative study. Finally, the third search (Search 3) investigated words surrounding mental health issues, especially self-esteem. The search links of ‘and’, ‘AND’, ‘OR’, ‘+’ were used in the appropriate programmes. The searches were carried out in electronic databases containing journal articles, books. Each group was searched individually with the final search combining all the terms in each group for a final, all-inclusive search. The search results are presented below in Table 2: Several results were immediately discarded as irrelevant. A total of 17 articles (out of 180) illustrated the connection between religious identity, level of practice and mental health. Additional findings/information gathered from current articles were added through research conducted over the following 24 months. Appendix 1 provides a list of the original articles identified by the search.
Source Psychinfo Medline (back to 1982) Web of Science
The structure of this review incorporates the interactions taking place in and between religious identity, level of religious practice and various aspects of mental health, especially self-esteem (Appendix 1). Interactions between the model components will be highlighted in order to illustrate the effects in a multidimensional framework. The six variables identified as common to the PC, M, and NP populations will be discussed individually, and in terms of their interaction with other model variables as illustrated in Figure 1.
DISCUSSION
Identity One of the easiest starting points for understanding the importance of a religious identity is to acknowledge that religious groups are social groups. BeitHallahmi (1989) proposed that religion is actually a system used to maintain identity, thus providing a bridge between individualistic and collective identity. This forms a direct link with the wellknown and heavily researched social identity theory (SIT) (Tajfel, 1978). In short, SIT proposes that members of a particular social group (the in-group) (e.g. Catholics, British, males) tend to see themselves in a more positive manner than members of other groups (outgroups) (e.g. Protestants, Australians, females). These categories make up our
social groups or social identities. This system of social comparison, along with group members’ biased assessments, results in a dynamic known as in-group favouritism. In-group favouritism can have positive outcomes, such as increased self-esteem and confidence, or negative repercussions, such as prejudice or segregation (Tajfel, 1978; Tajfel & Turner, 1986). In-group favouritism can lead, in turn, to the ultimate attribution error (Hewstone, 1990; Pettigrew, 1979). The ultimate attribution error is the tendency to justify the behaviour of one’s group while actively condemning the behaviour of other groups or individuals outside of one’s group. If, for example, one’s in-group takes part in what could be seen as a violent or immoral activity, the justification for the behaviour will be found within the environment or outside forces and influences. However, if an outgroup takes part in those very same activities, the out-group is likely to be condemned for acting on their selfish, immoral internal urges (Hewstone, 1990; Loewenthal, 2000; Pettigrew, 1979; Tajfel, 1978). When put into the context of religion, Loewenthal (2000) claims that SIT has both pleasant and unpleasant implications. The most obvious positive aspect of religious group membership is the social support network and increased feelings of value and uniqueness one gains by joining the group. The individual will experience a sense of belonging or membership. Religious identity can actually increase in times of illness or difficulty, thus highlighting the importance of the religious group as a social support network as well as a possible coping mechanism (Blaine & Crocker, 1995).
Loewenthal (2000) highlights examples of liberation and terrorism where the in-group (the group to which one belongs) is fighting for basic human rights and freedom regardless of methods. Meanwhile, the out-group (any group one doesn’t belong to) is seen as terrorists, religious vigilantes, monsters and baby-killers. Putting this into real-life terms, studies on the most salient social identities, the religious identities, of those caught up in the strife between the Protestants and Catholics in Northern Ireland have demonstrated that violence by one’s own group is viewed as defensible and provoked by external factors. Meanwhile, violence by the other group is seen as indefensible and unprovoked or as a moral failing within members of the out-group (Hunter, Stringer & Watson, 1991; Lewis, 1999). Repeated findings have also suggested that religious affiliation and attendance appear to have a strong link with higher scores on measures of authoritarianism and prejudice. This seems to contradict the core teachings of many religious groups, which emphasise good deeds, love and forgiveness (Argyle & BeitHallahmi, 1975).
Model interactions: Religion and identity If religious groups are social groups, it seems fair to suggest that religious identity can act as a form of social identity. Religious identity can be composed of, or interact with other forms of identity. One of the key areas of overlap appears to exist between ethnic identity, specifically cultural identity, and religious identity. Research suggests that religion has different outcomes depending on the ethnic or cultural group, to which one belongs. Cultural identity is a transient form of ethnic identity. In order to clarify the
distinction, ethnicity will be defined as, ‘A national or racial group of people’ (Cambridge Dictionaries Online, 2002). Culture will be defined as, ‘The way of life, especially the general customs and beliefs, of a particular group of people at a particular time’ (Cambridge Dictionaries Online, 2002). Clearly, one can maintain the same ethnic identity, based on nationality or race, while re-defining the cultural aspect of that identity if the beliefs and practices of the individual change to conform with the environment.
Model interactions: Religious identity and cultural identity Cultural and religious identities often overlap and appear to be intertwined. An individual’s culture can determine the religious doctrines he or she will be exposed to and individuals often define cultural groups by their religion. For example, Markstrom, Berman and Brusch (1998) investigated the religious identity/culture interaction and found that more religious individuals are more likely to report a greater ethnic identity. However, members of some social groups believe that their religious and cultural practices offer different, sometimes contradictory, ways of defining themselves (Jacobson, 1997). This begs the question: does religious identity still have an effect on personal well-being and mental health when it is distilled from the culture in which it has become enmeshed? Religious group membership may very well have the power to influence overall mental health when it is removed from the cultural context. While exploring the reasons why religion is a often seen as a more significant source of social identity when compared to ethnic identity, Jacobson (1997) found that some groups actually benefit from their struggle to separate their ethnic or cultural identity from their religious identity. In this study, a group of second-generation British Pakistanis was thought to demonstrate a growing tendency to accentuate a distinction between their Islamic (Muslim) religion and their Pakistani ethnicity as sources of identity. The youths viewed their ethnicity as a confining aspect of life relating to a particular place and set of non-religious customs and increasingly defining Islam as a universally relevant set of beliefs and rules that bypassed the limits of their culture. Jacobson concluded that young British Pakistanis were increasingly differentiating between their religion and ethnicity. They claimed that their religion played a more significant part in their lives in comparison to the influence of their ethnic background. The added focus on religious practices provided the youths with a method of dealing with the ‘ambiguities and contradictions’ (p.254) found in their social environment (Jacobson, 1997). An analysis of the literature (Appendix 1) indicates that religious identity does have an effect on levels of well-being, regardless of, and sometimes in spite of, cultural/ethnic influences. The strength of the effect appears to vary, depending on the ethnic group and the type of identity measured, but it is clear that social identity has an important influence on religious identity and mental health.
Model interactions: Religion, identity, race and self-esteem Religious identity can still influence overall well-being when removed from its cultural constraints, as illustrated by Jacobson (1997). Could the influence
also work in the opposite direction, allowing the ethnic practices and beliefs of religious group members to influence levels of religious identity? Racial identity is another form of ethnic identity. Unlike cultural identity, racial identity is not transient. Individuals maintain their racial identity regardless of the culture or religion to which they belong. Race is defined as, ‘A group of people with particular similar characteristics, who are considered as belonging to the same type, or the fact of belonging to such a group’ (Cambridge Dictionaries Online, 2002). Like cultural identity, racial identity can form a foundation element of religious identity. Blaine and Crocker (1995) investigated the effect of religious group membership on different racial groups practising within the same culture and faith. Does religious identity affect mental health (well-being) differently between different racial groups within the same faith? It has been suggested that members of minority groups may rely on religious groups to heighten their levels of self-esteem (Loewenthal, 2000; St. George & McNamara, 1984). Blaine and Crocker (1995) tested this theory, suggesting that, ‘The relationship between religious belief and psychological well-being should be more positive among Black than among White individuals’ (p.1031). Previous research suggested that Blacks are generally more religious than Whites which prompted the researchers to ask why this was so. Blaine and Crocker (1995) proposed that this relationship would be mediated by the social psychological components of religion. For example, increased feelings of value and uniqueness created by group membership would enable religiousness to act as an adaptive psychological function.
Blaine and Crocker’s (1995) questionnaire study found that religious belief salience and psychological well-being were positively correlated but this positive correlation existed only for the Black population. The salience of religious belief was also positively correlated with increased levels of self-esteem and life satisfaction within the Black population. This supports the theory that religious identity does affect well-being differently between racial groups of the same religion. Blaine and Crocker (1995) questioned why this relationship existed. Religion is positively associated with reported well-being in Black populations (St. George & McNamara, 1984). The most convincing explanation for the positive correlation in the Black population suggests that religion acts as a coping mechanism despite the findings suggesting, ‘Blacks face objectively worse circumstances than Whites’ (Blaine & Crocker, 1995, p.1033). Blaine and Crocker (1995) suggest that belonging to a religious group contributes to the development of a positive social identity and holding a religious belief system enables individuals to find explanations and gain new insights into events and situations that offer unsatisfactory explanations. This, in turn, enables Blacks to cope with their negative life circumstances. The added sense of control created by gaining new insights, one of Batson et al.’s (1993) Seven Conceptions of Mental Health, helps to enhance levels of self-esteem and self-perception. This, in turn, possibly influences the positive association between religion and well-being in St. George and McNamara’s (1984) study. The cognitive strategies involved in gaining this understanding, sense of control and heightened self-esteem can
be predictors of successful coping and mental health (Blaine & Crocker, 1995). This theory is upheld by Ressler’s (1997) report of a small but significant positive relation between scores on three wellbeing scales (Belonging, Optimism and Self-acceptance) and two aspects of religious identity (Activism and Religiosity). Ferraro (1998) supports this with the finding that religious practice is associated with all levels of well-being. Overall, it appears that religious identity does have an effect on mental health and the effect appears to be predominantly positive despite attempts at extracting religious identity from cultural influences and racial influences from religious identity.
Mental Health The relationship between religion and mental health It has already been suggested that it is important to define mental health variables within their cultural context. Conceptions of mental health vary crossculturally and all cultures have developed methods of treating mental disorders. This suggests that every culture has developed certain criteria for distinguishing sanity from pathology within their own cultural framework. The qualitative study related to this review identified self-esteem as a common issue or concept across three populations. The fact that self-esteem interacts with each of the model variables (Figure 1) on one level or another demonstrates that it is still necessary to discuss the importance of self-esteem as a key variable in maintaining positive mental health.
Self-esteem Why does an association between religion and mental health exist? Social identity theory suggests that religious group membership acts to increase feelings of self-worth, thus increasing levels of self-esteem (Hunter, Platow, Howard & Stringer, 1996). Self-esteem is the evaluative component of the self-concept. The self-concept is understood in broader terms since it acts as a representation of the self that takes in cognitions, affective aspects, behavioural and evaluational aspects of ourselves (Blascovich & Tomaka, 1991). Generally, self-esteem is believed to have both adaptive and selfprotective functions. Self-esteem has been related to various aspects of health and health-related behaviour, enabling researchers to establish it as a measurable mental health variable. It can also be viewed as an influential factor in promoting health-related behaviours such as exercise (Liao, Hunter & Weinman, 1995; Vingerhoets, Croon, Jeninga & Menges, 1990), eating a healthy diet or using birth control (Herold, Goodwin, & Lero, 1979). Abood and Conway (1992) found a relationship between self-esteem, health values and general wellness behaviour.
Religious orientation How do different approaches to religious belief affect mental health? Individuals belong to religious groups or hold religious beliefs for a variety of different reasons. Some may truly find comfort in their belief of the doctrines of their faith, while others may seek the company of like-minded individuals and familiar ceremonies at the end of a busy week. Some individuals turn to religious beliefs and ceremonies after trying everything else and still failing to find answers to life’s existential questions. Since humans do not function in a social vacuum, religious group membership, regardless of motivation, does have an effect (positive or negative) on overall mental health.
Batson and Ventis (1982) identified the Means, End and Quest religious orientations as measures of religion and mental health2. In general, means (extrinsic) oriented individuals exhibit little serious regard for answering life’s existential questions. It is seen as an immature orientation. Conversely, religious beliefs give meaning to the lives of ends (intrinsic) oriented individuals. Finally, the quest orientation envelopes individuals who are actively seeking but have yet to find acceptable answers to life’s existential questions. These orientations were applied to the seven conceptions of mental health (Table 1) defined by Batson et al. (1993). Overall a review of 197 findings from 61 different studies found that the means orientation had a predominately negative relationship with mental health; the ends orientation had a predominantly positive relationship with mental health; and the quest orientation revealed mixed results (Batson et al., 1993). Empirical evidence has been unable to uncover a clearly positive relationship between the means orientation and the seven mental health criteria (Table 1). Evidence exists for a clearly negative relationship with appropriate social behaviour; freedom from worry and guilt; personal competence and control; and open-mindedness and flexibility. It appears that the means orientation is likely to have a negative effect on mental health. Ventis (1995) identified the ends orientation as the more positive orientation. The ends orientation relieves existential anxieties, uncertainties and doubts. Batson and Ventis (1982) found it to be positively associated with appropriate social behaviour; freedom from
2 Based on Allport and Ross’s (1967) classical
worry and guilt; sense of personal competence and control; and personality unification and organisation when applied to the seven conceptions for mental health. Finally, researchers in the psychology of religion are still unable to assume a clearly positive or negative interaction between the quest orientation and mental health. Thus far, it appears that the quest orientation is positively associated with openmindedness and flexibility; negatively associated with absence of illness and freedom from worry and guilt; and either positive or neutral in association with personal competence and control, and self acceptance and self-esteem. Ventis (1995) attempted to explain these contradictions by stating, ‘The intellectual honesty and openness to religious questioning implied in this dimension may yield a sense of self-esteem and self-control, but at a possible price of personal unification and organisation, and continuing encounter with existential anxiety, worry, and/or guilt’ (p.41). Batson et al. (1993) concluded that the relationship between religion and mental health depends on both the measure of religion and the measure of mental health. This is a possible explanation for the variation in past results (Ventis, 1995). It is also important to remember that these three orientations represent very different ways of dealing with the basic existential questions in life (Batson et al., 1993). Out of the three types of religious orientation, quest was associated with identity confusion, while means oriented individuals defined an idealistic religious identity. Both have been viewed as a reflection of the strength of religious identity (Watson, Morris, Hood, Milliron & Stutz, 1998). Therefore,
distinction of extrinsic and intrinsic religiosity.
means and quest religiosity measures can be useful in assessing the level of religious identity of an individual. A quantitative study evolving from the combined outcome of this systematic review, as well as the afore-mentioned multi-faith qualitative study used Batson et al.’s (1993) External, Internal, and Quest scales of the Religious Life Inventory as one of the overall measure of religious identity. The correlations existing between the means and ends orientations, as well as means and quest religious orientations suggest that the three forms of orientation can be combined to create an overall measure of religious identity. Additionally, past results have suggested that the value identified as forgiving is one of the three values known to discriminate between the orientations (Tate & Miller, 1971). Interactions involving forgiveness, guilt and religious orientations will be discussed later in the review. These interactions suggest that particular religious orientations should and do have differing specific implications for mental health. Ventis (1995) suggested that the study of religious orientation and mental health needs to pay more attention to non-religious individuals in order to see the whole picture. Non-religious individuals are frequently the healthiest group but their data is often excluded or ignored in the psychology of religion.
Model interactions: Religious practice and mental health The bulk of religious research in the field of psychology tends to emphasise group belonging and psychological well-being rather than the effect of belief systems on physical health. It is also important to note that there have been many nonpsychology based medical studies analysing the relationship of physical health and religious group membership. This interest in the effects of religion on physical health suggests that a health/mental health connection could help explain the interaction between religion and mental health (Cinnirella & Loewenthal, 1999; Ellis & Biglione, 2000; Ferraro & Albrecht-Jensen, 1991; Frank & Kendall, 2001; Koenig, George, Hays, Larson, Cohen & Blazer, 1998; Levin & Vanderpool, 1987; and Levin & Markides, 1986). Body weight (Ellis & Biglione, 2000; Ferraro, 1998), blood pressure (Koenig et al., 1998), adult health (Ferraro & Albrecht-Jensen, 1991), adolescent health (Frank & Kendall, 2001) and coping with terminal illness (Levin, Wickramasekera & Hirshberg, 1998) are often identified as areas in which the health/mental health connection can be seen interacting with religious identity and levels of practice.
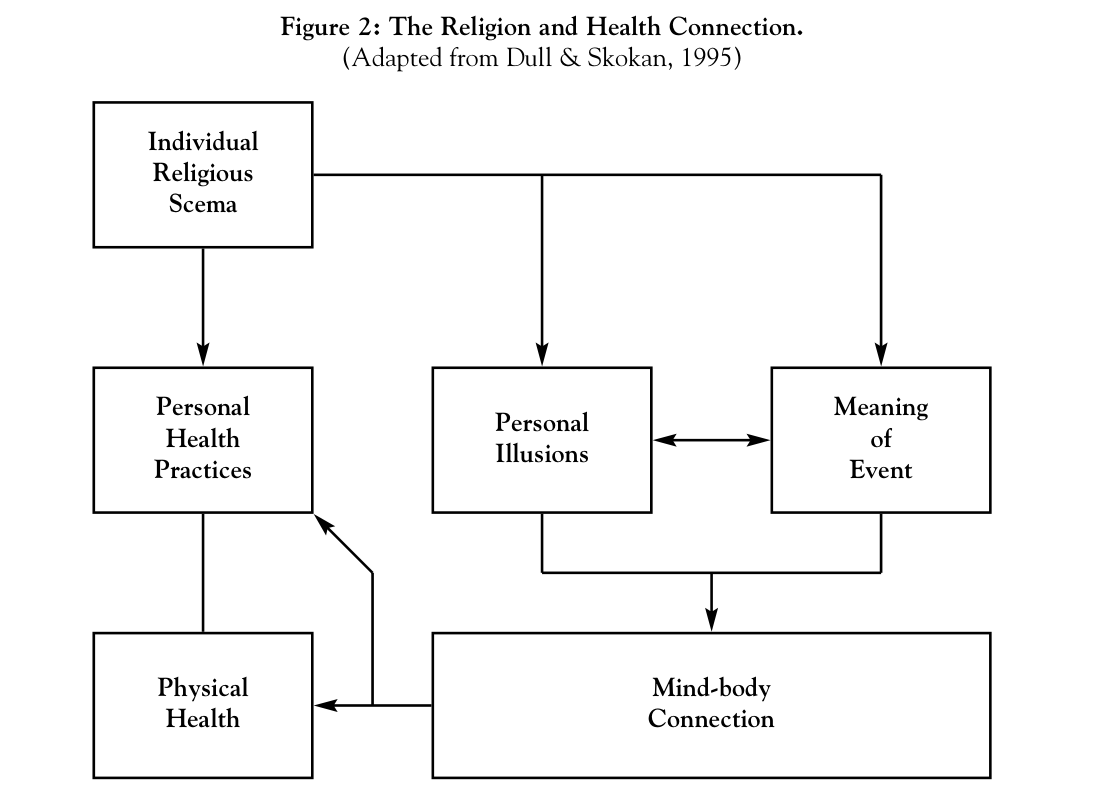
The Mind-body connection. Dull and Skokan (1995) proposed a cognitive model of religion’s influence on physical health in order to understand the changes found in mental health. They hypothesised that cognitions within religious belief systems may be associated with bodily changes in the immune system, thus leading to particular health outcomes. Religious belief systems can be viewed as the master motive (Allport, 1966), a superordinate schema (Rosenberg & Gara, 1985) or central attitude (Rokeach, 1960) when placed in the context of social cognition (Dull & Skokan, 1995). It is clear that religion can become a very powerful force when linked with social cognition. Dull and Skokan (1995) posed that, ‘Beliefs and ways of interpreting the world are more important to the study of religion’s effect on physical health than consideration of
group identity in isolation of other factors’ (p.51). Figure 2 presents an adaptation of Dull and Skokan’s (1995) cognitive model of religion’s influence on physical health, enabling researchers to distinguish between religion, a view or philosophy of life (e.g. Individual Religious Schema, Personal Illusions, and Meaning of Event), and group identity (e.g. Baptist, Catholic and Jewish). This allows individuals to identify themselves with a particular religious group (e.g. Baptist) simply because they were born into it, while taking into consideration that individuals could be either practising or non-practising. Dull and Skokan (1995) suggest that religious cognitions and beliefs can permeate all aspects of daily life, thus
increasing health benefits by following religious prescriptions. For example, religious groups prescribe beneficial health behaviours by creating rules against behaviour that could cause health risks. Eating (e.g. Kosher, fasting), drinking (e.g. no alcohol) and rules regarding sexual behaviour are excellent examples of the areas in life to which religious rules can be applied. This is supported by Koenig, Pargament and Nielsen’s (1998) suggestion that certain types of religious coping are strongly related to better health styles than nonreligious coping types, with negative religious coping behaviours being related to poorer physical health, worse quality of life and greater depression. Additionally, Comstock and Partridge (1972) found that higher levels of church
attendance are associated with less heart disease, emphysema, cirrhosis, tuberculosis and cancer of the cervix. Another way in which religious cognitions affect both physical and mentalhealth can be understood in the way that cognitions affect stress appraisal and physiology (e.g. terminally ill patients placing their trust in God and belief in the afterlife). It can also be observed in situations where religious cognitions appear to counteract a negative health risk. For example, Ferraro (1998) found that religious individuals tended to be more overweight than nonreligious individuals but failed to suffer the effects of low self-esteem, etc., that went along with obesity. Did the support system offered within religious group membership cancel out the loss of selfworth by reinforcing acceptance? Benson and Spilka (1973) also found support for the role of cognition in affecting the interplay between religion and mental health. They attempted to predict that believers’ levels of self-esteem and locus of control would influence their understanding (definition and description) of God. Out of a sample of 128 Catholic participants with similar religious backgrounds, Benson and Spilka (1973) found that self-esteem was positively related with positive images of God, such as loving and accepting Godimages, and negatively related to rejecting images. However, locus of control was unrelated to controlling beliefs. The researchers concluded that self-esteem might be a major determinant of God-images. Conversely, low self-esteem could cause an individual to reject God concepts. Dull and Skokan’s (1995) mind-body connection offers an interesting view of the way in which religious group identity and religious practice affect overall physical health by influencing cognitions. The mind-body connection appears not only to affect physical health but also to have very obvious effects on overall mental health (Benson & Spilka, 1973; Ferraro, 1998; Koenig, Pargament & Nielsen, 1998). The evidence found in support of the model can be used as an argument for the influence of religious identity and religiosity on levels of mental health, specifically self-esteem.
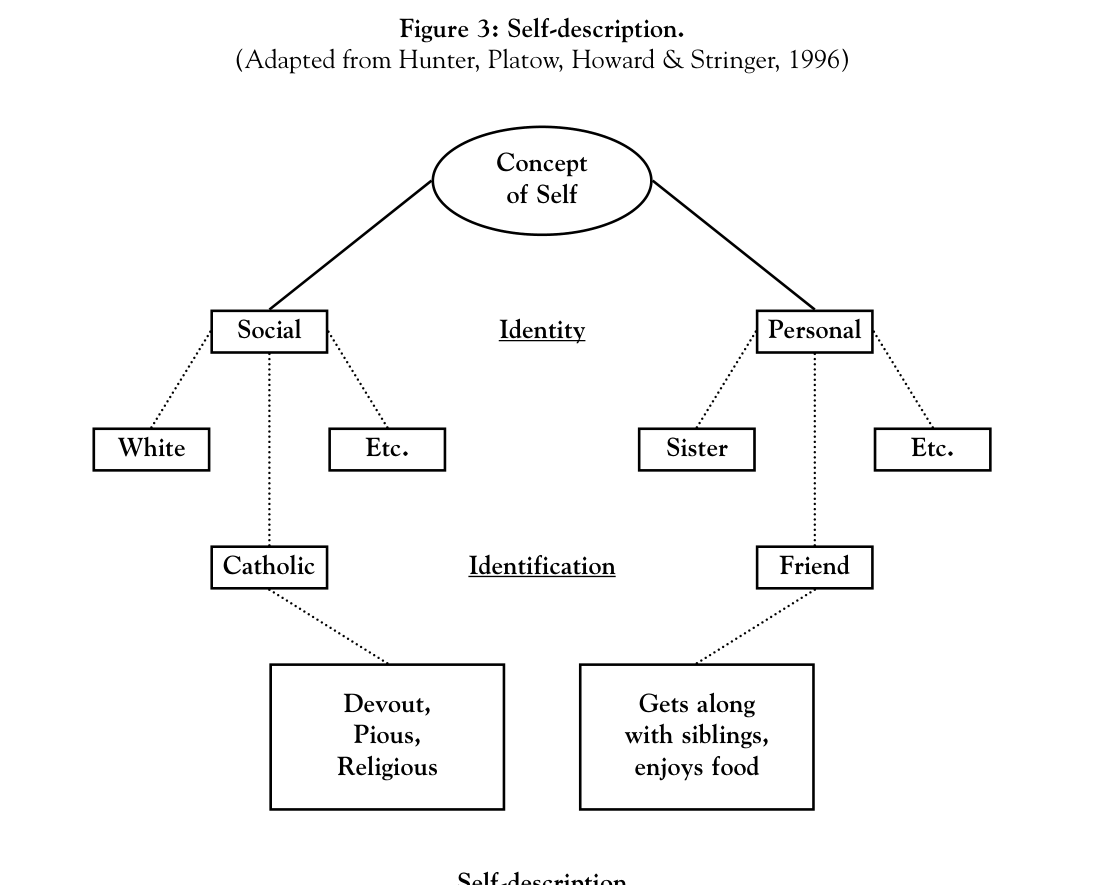
Model interactions: Religious identity and mental health Hunter et al. (1996) supported Dull and Skokan’s (1995) idea of re-defining the effects of religious group membership on mental health. They believed that the concept of self could not be adequately understood if its multi-dimensionality was ignored. Identity can be broken into social identity and personal identity, depending on the environmental demands. SIT suggests that a link exists between self-esteem, or an individual’s self-concept and levels of intergroup discrimination. Kirkpatrick (1998) offered support for this link, in terms of religion, with findings suggesting that positive models of self and others related to positive images of God and perceived relationships with God. Figure 3 provides a modified version of Hunter et al.’s (1996) multidimensional model of selfdescription. Hunter et al. (1996) explored the interaction between self-esteem (self-concept) and discrimination. Like Dull and Skokan (1995), they proposed the use of multidimensional measures of self-esteem in order to avoid losing the complexity in unidimensional models. Hunter et al. (1996) also recommended measuring self-esteem both before and after the manifestation of intergroup evaluative bias. The proposed model is
ideal for the study of interactions taking majority of positive effects on mental place between religious identity and health in normal populations with the mental health because it allows negative effects relating to obsessionality individuals to define their personal iden- and possible psychosis in clinical populatity. It also allows individuals to define tions. If religious identity and belief have the way in which others see them. such strong effects on mental health, it is Within this model, religious belief important to consider the effects that systems, or cognitions, interact with religious behaviour has on mental health religious identity in order to influence since religious behaviour can be an mental health. A review of the literature expression of both religious belief and suggests that these interactions have a identity.
Devout, Gets along Pious, with siblings, Religious enjoys food
Religiosity (religious practice) It is impossible to ignore the importance of social identity and group membership in terms of the effect of religious identity on levels of mental health. The following discussion explores interactions with another variable within the model (Figure 1), religiosity. How does religious identity affect mental health if two groups, belonging to the same religious organisation, have different levels of practice and commitment? Will the members of one group experience higher levels of stress, shame or guilt than the other group? Will the coping strategies for the religious group work equally as well on both the Orthodox and the less Orthodox in overcoming these stresses brought on by their religious identities? Religiosity is a concept that is widely understood but difficult to operationalise. Some researchers choose to measure religiosity in the form of religious behaviour or beliefs (e.g. prayer, attendance, fasting, etc.). Others, such as Glock and Stark (1965), felt that this method was too vague. They chose to conceptualise religious behaviour or activity, and thus religiosity, in five different dimensions. Dimensionally, religiosity could be described in terms of experiential activity; ritual activity; belief; intellectual activity; and the application to daily life. Loewenthal (1995) claims that some of these dimensions are still too difficult to operationalise. Therefore, she proposes three general measures of religiosity: affiliation; identity or self-definition; and belief in God (Loewenthal, 1995, p.4). There are ‘good’ forms and ‘bad’ forms of religiosity as far as positive and negative effects on mental health are concerned. For example, Brown and Prudo (1981) found that more religious individuals (assessed by church attendance) were less likely to suffer depression. Loewenthal (1995) explains this by suggesting that religiosity may have a positive affect on mental health because of the social networks provided by greater levels of church attendance. She also notes the favourable effects of belonging (group membership) on self-esteem and the feelings of spiritual support generated by religious group membership in times of need. Conversely, negative aspects of religiosity can lead to self-righteousness, which is in direct conflict with Batson et al.’s (1993) seventh requirement for mental health, open-mindedness and flexibility.
Model interactions: Religiosity and self-esteem The religious rules that the young people chose to follow in the previously discussed Jacobson (1997) study are known as boundaries. Boundaries are used to prevent groups from overlapping (Loewenthal et al., 1997). Boundary maintenance refers to activities that help maintain a separation between groups or individuals and one belief system or another. Loewenthal et al. (1997) suggested that the general reduction in stress attributed to religious group affiliation could be partly explained by the effect of boundary maintenance. They explored the effects of boundary maintenance on religious identity, levels of religiosity and mental health by examining the levels of stress found among two groups of Orthodox Jews believed to differ ‘in the strength of the boundary of their religious group’ (Loewenthal et al., 1997, p. 200). This study was also used to assess if the stresses and tensions of maintaining boundaries had any effect upon mental health. The results were then compared to related work containing church-going and non-practising Christians.
The Jews studied were recruited from ‘traditionally’ and ‘strictly’ orthodox synagogue membership lists in Britain during the 1990s. The key contrast between this study and related work in the field was found between orthodox Jews, practising Christians and nonpractising Christians. The comparisons showed that religious identity does have an effect on well-being. Boundary maintenance events were higher among the religiously active (e.g. orthodox Jews; practising Christians) whose members tended to report a higher level of religious observance. In short, the groups reporting high levels of religious activity reported higher levels of boundary maintenance, which increased anxiety. However, the orthodox Jews and practising Christians also reported low levels of disruptive events, which, in turn, lowered depression. Therefore, individuals with high levels of religious activity are more likely to suffer from anxiety than depression, despite the increased levels of boundary maintenance. Once again, religious identity, with its link to religiosity, seems to control for the negative aspects of maintaining religious group membership by decreasing levels of depression. While religious group membership may actually increase the levels of stress in religious individuals due to the costs of boundary maintenance, higher levels of religious belief and practice serve to decrease other stressors and may buffer the effects of stress (Blaine & Crocker, 1995; Loewenthal et al., 1997). This buffering effect could be partly caused by the increased levels of self-esteem that are synonymous with a positive social identity and increased sense of control. However, increased levels of stress in religious individuals are not exclusively attributed to the higher cost of boundary
maintenance and exposure to life stressors, nor is the buffering effect of religious group membership confined to that arena. There are other ways in which religious identity and religiosity can influence well-being. Koenig, Pargament and Nielsen (1998) showed that certain types of religious coping styles are more strongly related to better health status than other religious coping styles. Additionally, Luyten et al. (1998) found no evidence for a negative correlation between religiosity and mental health.
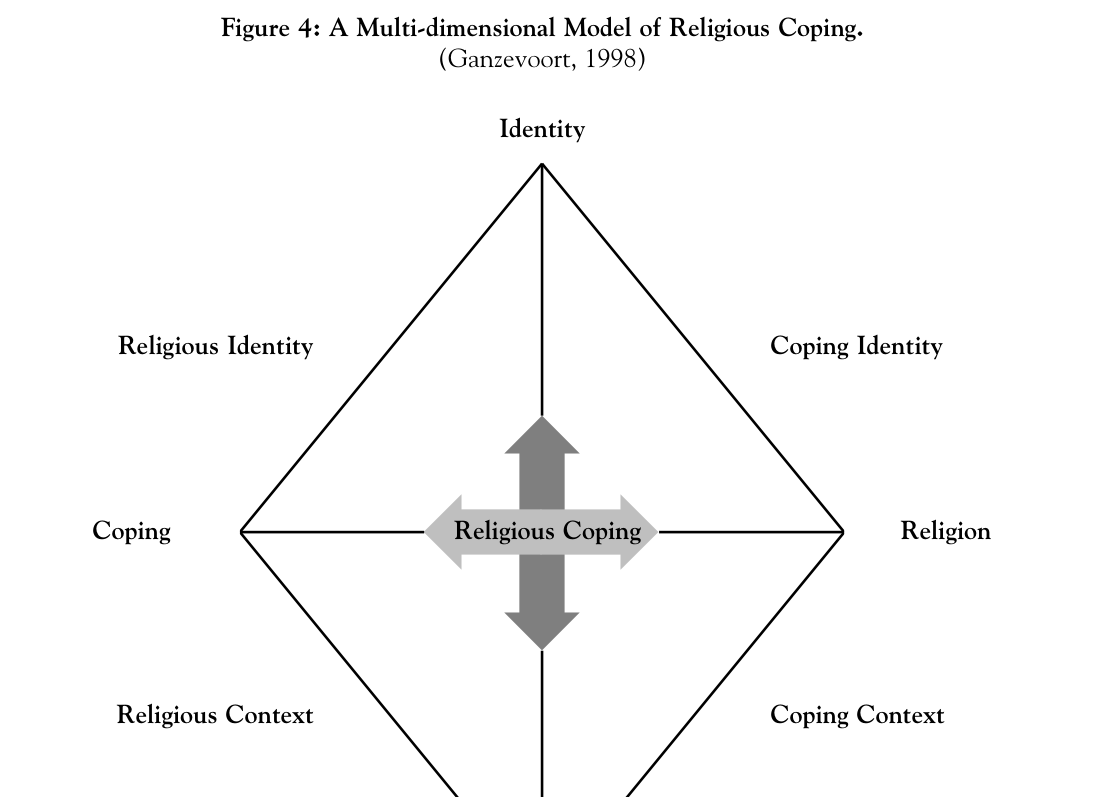
Model interactions: Religious identity, level of practice and mental health Ganzevoort (1998) illustrated the way in which religious identity and levels of practice buffer the effect of stress on mental health. He did this by establishing a comprehensive way of discussing identity while viewing religion as a functional coping mechanism within a multi-dimensional model. Ganzevoort (1998) believed that religion could influence all parts of the coping process or be the result of the coping process. Viewing this interaction as a bi-directional process (e.g. religion affecting coping, and coping affecting religion) suggests that religion acts as an unstable system that changes over time. Figure 4 presents Ganzevoort’s (1998) multi-dimensional, bi-directional representation of the way in which religious identity, level of practice and mental health interact in terms of coping. The religious coping interactions take place on the horizontal axis from the left side to the right side of Figure 4. Ganzevoort (1998) suggests that, within the crisis and coping process, interactions take place in and progress through five phases known as: (1) event; (2) event appraisal; (3) resource appraisal; (4) coping activities; and (5) coping
outcome, as well as the second central constant reformulation, continuously process, religion. Additionally, two other interacting with coping, religion and domains that act as cornerstones in the social context. Likewise, Blaine and process are known as: (1) the identity Crocker (1995) highlighted the imporprocess; and (2) the social process. The tance of the identity process in religious interaction between these two processes coping by identifying the formation of a can be seen on the parallel axis within positive social identity as one of the key Figure 4. benefits of religious group membership The identity process is best described for their Black Christian population. as the constant reformulation of the The social process represents the individual as he or she wants to be seen social context in which these interacby society as well as his or her own self- tions take place. In short, it offers a concept. Identity is a dynamic process in constantly changing playing field for the
Religious Identity Coping Identity ➡ ➡ ➡ Coping Religious Coping Religion ➡
Legend: ➡ ➡ Social Identity ➡ ➡ Context Religious Coping
process of coping, religion and identity. Crisis and coping, religion, identity and context should be seen as a complete dynamic process capable of interacting and developing over a life-span with each factor having the power to influence the other factors.
Perceived efficacy and religious practice between groups Beliefs about the effectiveness of religious forms of coping are thought to have a stronger effect on other behaviours than actual efficacy. Data collected from interview studies (Cinnirella & Loewenthal, 1999; and Loewenthal & Cinnirella, 1999) suggested that prayer was seen as an effective way to decrease depression in women compared to the use of medication and psychotherapy. Prayer was also identified as the most widely supported effective religious form of coping intervention. Muslims and Black Christians were more likely to believe in the efficacy of prayer when compared with White Christians, Jews and Hindus. Information gained from previous studies led to the formulation of a qualitative study investigating the perception of the efficacy of six types of religious coping behaviour (i.e. faith; prayer; keeping up with religious practices; attending a place of worship; consulting religious leaders and; praying for the sufferer) by different groups (Loewenthal, Cinnirella, Evdoka & Murphy, 2001). Loewenthal et al. (2001) posed that there is an overall positive relationship between several aspects of religiosity and mental health variables. However, it was noted that more specific measures of religion show a variety of relationships, ranging from positive to negative. In fact, a review of 30 studies carried out by Pargament (1997) found that religious
coping was commonly used to reach both negative and positive outcomes as the individuals searched for significance. Loewenthal et al.’s (2001) key question by-passed the conundrum caused by conflicting coping data and simply asked, ‘Regardless of whether and when religious coping actually ‘works’, what do people expect of religious coping’ (p.293)? Is religious coping seen as helpful and are some forms seen as more helpful or effective than other forms of coping? Loewenthal et al. (2001) found that the participants saw religious coping as relatively ineffective. However, when broken into religious and non-religious groups, religious individuals saw religious coping activities as somewhat effective. Prayer was seen as less effective than medication or psychotherapy in this study, whereas it was seen as more favourable than medication or psychotherapy in the previous qualitative study. Loewenthal et al. (2001) suggest that contradictory findings might be the result of the use of different methodologies. Out of the religious coping activities, prayer and faith were seen as the most effective forms of religious coping. In terms of depression, participants reported that overall faith and prayer were the most effective forms of coping. Maintaining religious practice and attending services were ranked as the second most effective forms of coping with religious leader consultation and praying for the sufferer being viewed as the least effective methods. Group differences in the beliefs about the efficacy of religious coping activities showed that the Muslims endorsed the effectiveness of every form of religious activity more strongly than the other groups. The Christians highlighted prayer and others praying for the sufferer
as more effective than the Jewish and religious ‘nons’, and the Jewish participants found the maintenance of religious practice, consulting a religious leader and others praying for the sufferer more effective than the Christian and religious ‘nons’. Overall, the religious ‘nons’ did not view religious coping as an effective way of dealing with their life difficulties. It is possible that cognitive factors could have had an important influence on coping behaviours and outcomes (Loewenthal et al., 2001). This supports Ganzevoort’s (1998) suggestion that religious interpretation affects the way in which individuals interpret events and the amount of influence a crisis has on faith depends on the phase of life in which the crisis takes place. Loewenthal et al. (2001) also support Dull and Skokan’s (1995) suggestion that cognitions (e.g. religious beliefs) help explain the mindbody connection between religious identity, levels of practice and mental health.
Shame and Guilt Do shame and guilt have an effect on religious identity and mental health? Research suggests that religious individuals leave themselves open to increased levels of shame and guilt compared to non-practising or less orthodox individuals (Bierbrauer, 1992; Fontaine, 1992; Hood, 1992; Hood et al., 1996; Richards, 1991; Vergote, 1988, and Watson, Morris & Hood, 1987). Nevertheless, religious individuals appear to be capable of overcoming the negative feelings associated with shame and guilt, despite the maladaptive effects on psychological well-being (Hood et al., 1996; Kabacka-Jasiecka, Dorcazk & Opoczynska, 1996; Maton, 1989; Pargament, 1997; Payne, Bergin, Bielema & Jenkins, 1992; van Uden & Peiper, 1996; Vergote, 1988). While religion, in general, has been known to emphasise guilt and sin, it also provides its followers with ways to overcome or diminish the maladaptive effects of guilt and shame (Luyten et al., 1998). Researchers experience difficulties in establishing a relationship between religious identity and psychological maladjustment caused by shame and guilt. Although both shame and guilt are negative emotions, it is important to distinguish between the two due to their different implications for interpersonal and intrapersonal functioning (Tangney, 1995; Tangney et al., 1995). Qualitative and quantitative studies have illustrated that guilt is viewed as the healthier component, whereas shame is viewed as maladaptive because it is associated with a negative view of the global self as well as a perceived loss of control. However, Jacoby (1997) suggests that shame might have a positive side to it, acting as the ‘guardian’ of dignity and thus protecting individuality and identity. Jacoby (1997) does support the idea that shame is the more negative component but only because of the way in which it manifests itself. Guilt is seen as causing negative feelings because of a bad action or thought, whereas shame has the power to make individuals feel completely worthless regardless of whether or not they have actually done something bad. This acknowledgement of the all-consuming power of shame led Jacoby (1997) to suggest that guilt acts as a defence mechanism against shame. The difficulty in establishing the connection between shame, guilt, religious identity, levels of practice and mental health lies in the fact that the tools available for measuring levels of guilt, such as the Test of Self-conscious Affect (TOSCA) (Tangney, Wagner & Gramzow, 1992) fail to measure severe
forms of guilt that are known to negatively affect healthy psychological functioning (Harder, Cutler & Rockart, 1992). Jacoby (1997), Tangney (1995) and Harder et al. (1992) suggest that, like shame, guilt can also become a maladaptive function. The difficulty of establishing a relationship between religious identity and psychological maladjustment is intensified when it is acknowledged that studies dealing with the psychology of religion mixed with the theology of guilt have actually been measuring the wrong component of guilt all along. In light of these findings, what is commonly called ‘guilt’ in the psychology of religion literature can actually be viewed as guilt mixed with shame (Lewis, 1971; Tangney et al., 1995; Tangney, 1996). Jacoby (1997) complicates the issue by suggesting that shame and guilt are actually sub-species of the master emotion, anxiety. This suggests that it is impossible to separate the two functions completely. How can researchers ensure that they are measuring the effects of shame and guilt on religiosity and mental health? Luyten et al. (1998) designed a four-part study that supported the theory that religious identity does have an effect on mental health by influencing levels of shame or guilt. The fact that shame and guilt are often fused together prompted Luyten et al. (1998) to focus on partialing out shame from guilt, and viceversa, in order to assess fully the unique effects of the negative forces. Luyten et al. (1998) found that shame and guilt have a profound effect on religious identity and mental health. In fact, it seems that religious identity is effective at smoothing out the maladaptive effects of shame and guilt. The researchers were unable to find evidence for a negative correlation between reli-
giosity and mental health despite the fact that religious individuals were more prone to guilt and reported more feelings of guilt. Their findings also suggested that religion could attenuate the maladaptive effects of shame. Luyten et al. (1998) warns that this review was correlational in nature and must be interpreted with caution, especially since, ‘It is very likely that there is a mutual influence between religiosity and mental health’ (p.180). Guilt does have an effect on the ways in which religious identity affects overall mental health, but the negative effects associated with guilt are controlled for when religions offer their members effective ways to cope with several kinds of psychological stress. This links directly back to the positive benefits of group membership proposed by SIT, as well as the range of religious behaviour and activity available as stress reducing options (e.g. prayer, confession, Hail Mary’s, etc.). Therefore, ‘It can be argued that religiosity can prevent and/or attenuate, cognitively and effectively, the negative effects of guilt and/or shame directly by providing believers with a sense of meaning, control and self-esteem’ (Luyten et al., 1998, p.169). Once again, these provisions are components of the Batson et al.’s (1993) seven conceptions for mental health.
Forgiveness (Grace) What is forgiveness and how does it function within a multi-dimensional model of religion? Forgiveness is the functional component of grace. In fact, grace can be described as an act of forgiveness. Without grace, however, individuals could not reap the mental health rewards of forgiveness. This symbiotic interaction can be clearly understood when placed within the Christian context. As
Christians, individuals are taught that they are expected to forgive others. In return, they can expect to be forgiven. They are also taught that God will give them the grace to accept forgiving and forgiveness as gifts. Genuine forgiveness must be voluntary and unconditional (Worthington, 1998). Prior to 1985, only five studies exploring forgiveness had been identified. After 13 years of increased research and interest in the scientific study of forgiveness, 1998 left scientists with a grand total of 55 studies. Few of these directly dealt with religion making it difficult to identify previous studies through a systematic analysis. Worthington (1998) proposed that forgiveness is a concept found in many religions across the globe yet it does not demand a religious context to exist. Forgiveness can be taught ‘through prayer, ritual, instruction, meditation, and parable’ (Worthington, 1998, p.165). The outcomes of forgiveness can be favourable. Throughout the 55 studies identified by Worthington (1998), forgiving behaviour showed statistically significant decreases in anxiety and depression and significant increases in hope and self-esteem. The decreases in levels of anxiety and depression correspond with Batson et al.’s (1993) freedom from worry and guilt component of mental health. Additional studies suggest that guilt-prone individuals might be more prone to forgive. Guilt might actually have a positive function when it comes to encouraging or motivating forgiving behaviour.
Model interactions: Forgiveness and religious identity In Western societies such as the US and UK, where more than 80 per cent of the public claimed to identify with God through their belief in Jesus Christ, it is not surprising that the concept of forgiveness plays a part in everyday life for many people. What kind of effect will issues of forgiveness have on the overall mental health of religiously inclined individuals? Gorsuch and Hao (1993) used a cross-sectional survey to examine the relationship between self-reported forgiveness and religious variables. They also attempted to determine whether forgiveness is best described as a unidimensional or multi-dimensional model. During this study, 15 religious items were identified as significantly important: self-identification items (e.g. Protestant, Catholic, Jewish, and no/other) as well as self-descriptions such as ‘born again’. The importance of religion in one’s life was assessed as well as religious group membership, attendance and intrinsic and extrinsic religious motivations. Results uncovered one higherorder forgiveness factor as well as four additional forgiveness factors: (1) Forgiving motive (measuring an underlying motive facilitating forgiveness); (2) religious response (measuring religious coping behaviours such as prayer); (3) forgiving pro-action (measuring movement toward the other person); and (4) hostility (measuring responses such as resentment, revenge, and self-justification) (Worthington, 1998, p.237). When the higher order effects were taken into account and the additional four factors were analysed as a group, Gorsuch and Hao (1993) found that they made a significant contribution to prediction of the religious variables. The findings suggested that: forgiveness levels could be a predictor variable for levels of religious identity and religiosity.
Likewise, religious identity and religiosity could be used to predict levels of forgiveness in a multidimensional model.
Model interactions: Forgiveness and religiosity Paloma and Gallup (1991) also focussed their study on religiosity and its relationship with forgiving behaviour by examining the relationship between forgiveness and well-being. They also analysed the influence of religious variables and prayer with forgiveness. The study implemented a cross-sectional survey to investigate forgiveness-related beliefs and behaviours such as religious salience, participation levels, beliefs and prayer. Results showed that 94 per cent of the participants ranked forgiveness in religious people as a fairly or very important quality. However, results from the study showed that only 48 per cent said that they usually attempted to forgive other people. Positive attitudes towards forgiving behaviour were related to life satisfaction, with life satisfaction being negatively related to resentment and positively related to praying for the offender. Support for the concept of grace was found when 83 per cent of the participants suggested that they needed God’s help truly to forgive someone, with only 15 per cent feeling that they could forgive of their own accord. Additionally, ‘positive correlations emerged between acts of forgiveness and prayer experience, religious salience, feeling close to God, being a born-again Christian, and meditative prayer’ (Worthington, 1998, p.277). This study suggests that the majority of people feel that forgiveness is an important aspect of religious life but only half of those individuals reported that they actively try to forgive others. Overall, forgiving behaviour has a slight
positive influence on life-satisfaction and thus well-being when linked with religious identity and religiosity.
Model interactions: Forgiveness, guilt and religious orientation Can the slight positive effects of forgiveness hold up to the detrimental effects of guilt and shame? Past results suggest that the value identified as forgiveness is one of the three values known to discriminate between the previously discussed (p.18–21) orientations (Tate & Miller, 1971). Meek, Albright and McMinn (1995) explored the relationship between religious orientation, individual experiences of guilt and forgiveness and subjective well-being with a crosssectional survey. Participants were asked to imagine three scenarios in which they were offenders. Compared to ends oriented individuals, means oriented individuals reported higher levels of guilt, less chance of repeating the offence, less satisfaction about getting away with the offence (e.g. getting the day off work), and a higher probability that they would confess. One hundred per cent of participants showed increased levels of guilt after telling someone else about the offence, and a decrease in guilt after envisioning a confession. After the confession scenario, those in the grace condition were more likely to feel better, in comparison to the no-grace condition. Additionally, means oriented individuals were more likely to forgive themselves and feel forgiven by God than ends oriented individuals. In short, guilt appeared to be the main factor in determining the differences in feeling good or bad about an offence between the means and ends orientations. This led Meek et al. (1995) to suggest that means oriented religious individuals are more susceptible to guilt than ends
oriented individuals. However, the means oriented individuals reported that they were more likely to confess their offence and demonstrated a greater likelihood that they would feel better after confessing, be able to forgive themselves and feel forgiven by God (Worthington, 1998). Meek et al. (1995) concluded that means oriented religious individuals were more guilt prone than ends oriented.
Model interactions: Forgiveness as a form of religious coping How does forgiving affect the overall mental health of individuals? Maltby, Macaskill and Day (2001) examined the relationship between forgiveness of self, forgiveness of others, personality and general health measures. The aims of this study were based on previous findings suggesting that forgiveness is an important factor in facilitating psychological well-being, especially in clinical settings (Heble & Enright, 1993; McCullough & Worthington, 1995). Past research also highlighted the importance of analysing the relationship between religious coping as well as forgiveness and empathy (McCullough & Worthington, 1995; McCullough, Worthington & Rachal, 1997; Pargament, 1997; Pargament & Rye, 1998). Mauger et al. (1992) found that failure to forgive oneself or others led to greater levels of psychopathology. Specifically, the failure to forgive oneself was ‘significantly positively correlated with depression, anxiety, distrust, self-esteem, and social introversion, while failure to forgive others is significantly positively correlated to schizophrenia traits, social desirability, self-alienation, and persecutory ideas’ (Mauger et al., 1992, p.882). This clearly suggests that failure to take part in forgiving behaviour, be it of oneself or others, has strong, negative implications for overall general health. Maltby et al. (2001) hypothesised that it should be possible to predict the expected relationships between forgiveness of oneself and others as well as measures of personality and psychological well being. Results for a non-clinical sample generally supported Mauger et al.’s (1992) findings, with a few exceptions. For both men and women, the failure to forgive oneself showed a significant positive correlation with negative mental health traits such as neuroticism, depression and anxiety. However, for men, the failure to forgive others had a significant negative correlation with extraversion and a significant positive relationship with depression. It is interesting to note that Maltby et al.’s (2001) study offered support for the negative relationship between failure to forgive others and depression. This suggests that there is some relevance to Mauger et al.’s (1992) findings that pointed to the possibility of individual failure to forgive others resulting in higher levels of depression. The female population demonstrated that failure to forgive others had a significant positive relationship with psychoticism, social dysfunction and depression. In contrast, Maltby et al. (2001) failed to find a significant relationship between forgiveness and social desirability. Each sex exhibited different forgiving behaviours in the forgiveness of others but not in the forgiveness of self. Maltby et al. (2001) proposed that this paradigm be analysed in greater detail during future studies. Forgiveness of self and others appears to have a positive effect on overall mental health and well-being. These findings also suggest that failure to forgive oneself or others could be detrimental to an individual’s overall mental health.
Model interactions: Forgiveness and religious identity How does forgiving facilitate coping in religious groups? Worthington (1998) suggested that, ‘Forgiveness is a method of religious coping for many people’ (p.60). Viewing forgiveness as a coping mechanism opens the door to a wellestablished area of research. Participation in small religious groups is believed to be positively related to forgiving behaviour (Wuthnow, 2000). This positive relationship may be maintained through the generation of different forms of capital, such as social capital, involved ingroup membership. Social capital is believed to strengthen bonds between group members, thus enhancing a sense of belonging, social skills and trust. The second form of capital gained from religious group membership, cultural capital, refers to the habits, interests and hobbies (e.g. music, literature) that give people a shared identity. This identity helps distinguish them from others, or the out-groups. Cultural capital is not believed to influence forgiving behaviour directly but it is seen as a way to influence group members’ self-worth, thus making them more trusting and optimistic about human nature. This trust, in turn, might make it easier for an individual to forgive members of his or her group (Wuthnow, 2000). Emotional capital, the third form of capital, relates to the emotional support gained from sharing personal problems with one’s group. Comparison of experiences and problems promotes forgiveness as group members learn from one another or recall facing a similar dilemma. Spiritual capital, the final form of capital, helps religious group members
distinguish between activities that are specifically related to the divine (Verter, 1998). Praying, singing, meditating and discussing religious texts are examples of ways in which spiritual capital is exhibited within religious groups. In the Christian faith especially, discussion of Biblical texts and prayer groups could expose group members to stories about people seeking and receiving forgiveness, as well as setting up a model of interacting with God, which can then be generalised to behaviour towards other people (Lawson, 1997). Wuthnow (2000) identified which type of capital had the greatest effect on forgiving behaviour. Respondents were asked if their religious group helped them forgive someone, healed their relationships or helped them towards relationship repairs. He found that: (a) over three-fifths of the respondents said that their small religious group helped them to forgive someone; (b) almost threequarters claimed to have relationships healed because of their group; and (c) approximately two-fifths said that their groups had helped them work towards relationship repairs. The length of time spent participating in the groups also increased the likelihood of giving positive responses to the three questions discussed above. Frequency of attendance was seen as an influential religiosity factor with members who attend less than once a month being less likely to answer positively to two of the three questions. Additionally, individuals who experienced higher levels of guilt were more likely to take part in forgiving behaviour. Activities involving emotional and spiritual capital showed strong positive relationships in influencing forgiving behaviour while social and cultural capital activities were unrelated. Wuthnow (2000) concluded that
forgiving behaviour was facilitated by group emphasis on prayer, sharing and learning about forgiveness. Wuthnow’s (2000) results demonstrate that religious group membership or religious identity has a strong positive effect on forgiving behaviour if the group facilitates the growth of emotional and spiritual capital. In the context of mental health, Wuthnow (2000) found that respondents who gave positive responses to the three forgiveness questions were also significantly more likely to claim that their small religious group encouraged them when they were feeling depressed and helped them overcome feelings of guilt. Measures of pro-social behaviour were also significantly related to forgiveness.
Summary and conclusions Thus far, the literature has established that there definitely is a relationship between religious identity, level of practice and mental health, especially self-esteem. However, the direction of influence in the underlying connections taking place in the relationship varies according to social group, racial group, cultural group, religious orientation or level of religiosity. Religious beliefs and religious identity influence the effect of shame and guilt on overall mental health, as well as the proneness to and mediating effects of forgiving behaviour in religious individuals. Taking all the variables into account, the literature leans towards favouring a positive association between religious group membership and mental health but a few of the studies suggest that effects are not always positive. Once again, these discrepancies make it difficult to progress to measuring and explaining the reasons for the interaction between religious identity, religiosity and self-esteem when researchers cannot predict exactly which form the interaction will take.
A comprehensive psychology of religion Pruyser (1987) accounted for these discrepancies by suggesting that the variations exist due to the multiple directions from which the psychology of religion can be approached. He suggests that the field of the psychology of religion has become so ‘diversified and subspecialised’ that it is difficult to fit all the methodological approaches and empirical findings under one heading. This was attributed to the fact that psychology itself offers multiple approaches to the study of religion (e.g. clinical, pastoral, developmental, social, etc.), while still being researched in theological and academic subjects completely removed from psychology. In addition, the phenomena of religion make this system even more complicated. In short: ‘What is being studied by any of the psychologies of religion, are also so diverse and often so systematised in their diversity, that we should no longer speak of religion at large, but of specific religions, faith groups, denominations, sects, cults, or individuals, perhaps even further qualified by adjectives such as liberal, orthodox, fundamentalist, evangelical, Hindu, Shiite, Sunni, capitalist, Marxist, Anabaptist, militant, pietistic, established, in free-church tradition, or what not’ (Pruyser, 1987, p.173). Pruyser (1987) also suggests that the different motivations of researchers in the psychology of religion contribute to the confounded findings. Some religious researchers set out to defend religion, while others tend to focus on deviant and controversial practices. Likewise, some
researchers attempt objectively to study subjective experiences in order to form a better understanding while others focus on the functions religion serves in human life. Clearly, a comprehensive psychology of religion is difficult to obtain because of the multitude of aims and approaches. Pruyser (1987) cites methodological and epistemological complications as one of the key causes and outcomes of the conflicted findings in the psychology of religion. A lack of consensus on conceptual outlooks, categories and theoretical frameworks leaves researchers without a clear guide. Religious findings are often regarded as demographic information (only!) in larger studies, making references and results involving religious variables difficult to find as part of a bibliographic database search.
Methodological concerns O’Connor (1998) clarifies the difficulties facing researchers in the psychology of religion. O’Connor analysed pre-existing literature reviews that attempted to summarise the relationship between religion and mental health (Argyle & BeitHallahmi, 1958/1975; Batson & Ventis, 1982; Batson et al., 1993; Becker, 1971; Bergin, 1983; Brown, 1994; Corveleyn, 1991; Dittes, 1969; Gartner, Larson & Allen, 1991; Lea, 1982; O’Connor, 1983; Payne, Bergin, Bielema & Jenkins, 1991; Sanua, 1969; Schumaker, 1992; Stark, 1971). These literature reviews surveyed psychological literature in the area of religion and mental health between the turn of the century and 1998. O’Connor (1998) found that many studies drew attention to various theoretical and methodological concerns. This present review also uncovered some methodological concerns identified by the authors. The concerns identified
by O’Connor will be linked with the findings of the present review and distilled into four key methodological issues. Those four areas are: (1) Definitions; (2) Religious groups researched; (3) Continued focus on one issue at a time; and (4) Measures. Suggestions for addressing the issues will be made. A brief proposal for addressing these issues in future studies will then be presented.
Definitions The complex issues involved in defining terms such as religious identity, religiosity and mental health have rarely been addressed in past research studies. It has already been suggested that it is important to define religion by its cultural context but the use of broad, general definitions enables researchers to apply measures and findings to large groups while compromising the level of understanding of the diversity of interactions.
Religious groups researched The majority of research has focused on Christian and Jewish, western religious populations. A brief glance at the literature suggests that most of the studies have researched varieties of Christian or Jewish religiousness. Ventis (1995) also suggested that the psychology of religion needed to broaden its scope by researching less traditional religious groups. Additionally, it is also important to study other world religions such as Islam, Hinduism, Buddhism, Sikhism, etc. Brown (1987) summarised the situation nicely when he stated, ‘Research in the psychology of religion should differentiate among religious persons, their beliefs and knowledge, attitudes and responses, claimed experiences, and the religious tradition of the group in which they live’ (p.208).
Continued focus on one issue at a time An over-reliance on simple, uni-dimensional models, simple correlations and linear causal explanations has failed to uncover the complex relationships existing between religion, identity and mental health. Past research often focussed on uni-dimensional interactions (e.g. religiosity and anxiety, religiosity and depression, etc.). While this information has successfully illustrated the relationships and underlying interactions between various aspects of religion and mental health, a call for more intricate multidimensional models exists, making the issue of developing working definitions even more important.
Measures
Psychologists of religion have been forced to rely on self-report measures. O’Connor (1998) suggests that it is possible that this reliance on the measurement model has led some researchers to claim too much on too little evidence. The effect that these claims might have on the understanding of the relationship between religious identity, religiosity and mental health becomes even more worrying if one takes into account the fact that past definitions, models and measurements might have been inappropriate. O’Connor (1998) also cites a general neglect of, ‘The personal-historical and socio-contextual variables…that pertain to, shape and influence a person’s experiences, reactions, responses, and language, either in religious or mental health terms’ (p.129).
Informed choices How can these methodological issues be addressed in future studies? Findings from past research studies can act as guides, mixed with the knowledge of existing methodological/theoretical issues. For example, keeping in mind that particular orientations to religion should and do have differing specific implications for mental health, future research should include a ‘non’ group (Ventis, 1995), as well as eastern religious populations. This would also allow newly developed and existing measurements to be extended to a variety of groups and cultures containing both religious and nonreligious individuals. Future projects could incorporate both qualitative and quantitative methods into a large-scale development of definitions and concepts common to most, if not all, religious and non-religious groups. Culturally sensitive and generic concepts could be added or excluded, depending on the populations in question for each study. Despite the time and effort involved in carrying out such a large-scale, multi-cultural study, results obtained through the combination of qualitative and quantitative data collection could ensure that the ‘right questions’ were being asked for each group studied in the psychology of religion. In short, developing a greater understanding of the perceived relationship, underlying interactions and definitions of relevant concepts might result in less contradictory findings in studying the effect of religious group membership on levels of mental health. A review of the literature suggests that it is difficult to find definitions and thus, measurements, acceptable to all religious and non-religious groups. A possible method of clarifying the confusion surrounding the variables represented in Figure 1 might involve openended interview studies devised to explore the understanding of these variables in more depth. A new causal framework could be proposed using the variables identified during this review or adding new variables generated from
additional qualitative interviews. As the interactions are studied in more detail, a bi-directional, multi-dimensional framework could be developed over time. For example, a model including the four components, identity, religiosity, shame and forgiveness could be linked to shared concepts or definitions of group, family, cultural or political group membership, etc. in order to better understand the influence of social identity. Likewise, the dynamic interactions of these variables could be linked with the study of moral reasoning in order to see if the level of emphasis placed on each variable relationship changes over time, based on group identity. Finally, questions generated during the current review, such as, ‘How important is the influence of religious identity and level of practice on overall mental health in religious and non-religious individuals?’ and, ‘Does religious identity have a greater positive or negative influence on social groups with different types or levels of religiosity?’, have been driven by previous findings in the psychology of religion. The methodological issues uncovered and discussed in the current review suggest that they should be explored both qualitatively and quantitatively, justifying the call for the development of a methodology based on evidence and intent on the progression of a psychological theory of religion.
References Abood, D.A. & Conway, T.L. (1992). Health value and self-esteem as predictors of wellness behaviour. Health Values: The Journal of Health Behaviour, Education, and Promotion, 16(3), 20–26. Allport, G.W. (1966). Religious context of prejudice. Journal for the Scientific Study of Religion, 5, 447–457.
Allport, G.W. & Ross, J.M. (1967). Personal religious orientation and prejudice. Journal of Personality and Social Psychology, 5, 432–443. Argyle, M. & Beit-Hallahmi, B. (1975). The social psychology of religion. London: Routledge & Kegan Paul. (Original work published in 1957) Argyle, M. & Beit-Hallahmi, B. (1997). The psychology of religious behaviour, belief and experience. London: Routledge. Batson, C., Schoenrade, P. & Ventis, W. (1993). Religion and the individual: A social-psychological perspective. New York: Oxford University Press. Batson, C.D. & Ventis, R.L. (1982). The religious experience: A socialpsychological perspective. New York: Oxford University Press. Becker, R.J. (1971). Religion and psychological health. In M.P. Strommen (Ed.), Research on religious development: A comprehensive handbook. New York: Hawthorne. Beit-Hallahmi, B. (1989). Prolegomena to the psychological study of religion. London: Associated University Press. Benson, P. & Spilka, B. (1973). God image as a function of self-esteem and locus of control. Journal for the Scientific Study of Religion, 12(3), Bergin, A.E. (1983). Religiosity and mental health: A critical re-evaluation and meta-analysis. Professional Psychology: Research and Practice, 14, Bierbrauer, G. (1992). Reactions to violation of normative standards: A cross-cultural analysis of shame and guilt. International Journal of Psychology, 27(2), 181–193. Blaine, B. & Crocker, J. (1995). Religiousness, race and psychological well-being: Exploring social psycho-
logical mediators. Personality and Social Psychology Bulletin, 21(10), Blascovich, J. & Tomaka, J. (1991). Measures of self-esteem. In J.P. Robinson, P.R. Shaver & L.S. Writghsman (Eds.), Measures of personality and social psychological attitudes. California: Academic Press. Brown, L.B. (1987). The psychology of religious belief. London: Academic Press. Brown, L.B. (1994). The self: Measurement requirements from an interactionist perspective. London: Academic Press Limited. Brown, G. & Prudo, R. (1981). Psychiatric disorder in an urban and a rural population I: Aetiology of depression. Psychological Medicine, 11, Cambridge Dictionaries Online (2002). Retrieved 20th February, 2002 from Cinnirella, M. & Loewenthal, K.M. (1999). Religious and ethnic group influences on beliefs about mental illness: A qualitative study. British Journal of Medical Psychology, 72, Comstock, G.W. & Partridge, K.B. (1972). Church attendance and health. Journal of Chronic Diseases, 25, 665–672. Corveleyn, J. (1991). Religion and mental health in the 80s: A survey and critical review. Paper presented at the Fifth Symposium for European Psychologists of Religion, Leuven, Belgium. DeHaan, L.G. & Schulenberg, J. (1997). The covariation of religion and politics during the transition to young adulthood: Challenging global identity assumptions. Journal of Adolescence, 20(5), 537–552.
Dittes, J.E. (1969). Psychology of Religion. In G. Lindzey & E. Aronson (Eds.), The handbook of social psychology (Vol. 5). Mass: Addison-Wesley. Dull, V.T. & Skokan, L.A. (1995). A cognitive model of religion’s influence on health. Journal of Social Issues, 51(2), 49–64. Ellis, L. & Biglione, D. (2000). Religiosity and obesity: Are overweight people more religious? Personality and Individual Differences, 28, 1119–1123. Ferraro, K.F. (1998). Firm believers?: Religion, body weight and wellbeing. Review of Religious Research, 39(3), 224-244. Ferraro, K.F. & Albrecht-Jensen, C.M. (1991). Does religion influence adult health? Journal for the Scientific Study of Religion, 30(2), 193–202. Fontaine, J.R.J. (1992). De inbedding van schuld en schaamte in culturele context: Een verglijkend onderzoek met Indonesische en Belgische studenten. [Guilt and shame in cultural context: A comparative study with Indonesian and Belgium students.] Unpublished master’s thesis, Catholic University Leuven, Belgium. Frank, N. & Kendall, S. (2001). Religion, risk prevention and health promotion in adolescents: A community-based approach. Mental Health, Religion & Culture, 4(2), 133–148. Gartner, J., Larson, D.B. & Allen, G.D. (1991). Religious commitment and mental health: A review of the empirical literature. Journal of Psychology and Theology, 19, 6–25. Ganzevoort, R.R. (1998). Religious coping reconsidered, Part One: An integrated approach. Journal of Psychology and Theology, 26(3),
Glock, C.Y. & Stark, R. (1965). Religion and society in tension. Chicago: Rand McNally. Gorsuch, R.L. & Hao, J.Y. (1993). Forgiveness: An exploratory factor analysis and its relationship to religious variables. Review of Religious Research, 34, 333–347. Harder, D.W., Cutler, L. & Rockart, L. (1992). Assessment of shame and guilt and their relationship to psychopathology. Journal of Personality Assessment, 59, 584–604. Heble, J.H. & Enright, R.D. (1993). Forgiveness as a psychotherapeutic goal with elderly females. Psychotherapy, 30, 658–667. Hewstone, M. (1990). The ‘ultimate attribution error’? A review of the literature on intergroup causal attribution. European Journal of Social Psychology, 20(4), 311–355. Herold, E.S., Goodwin, M.S. & Lero, D.S. (1979). Self-esteem, locus of control and adolescent contraception. Journal of Psychology, 10(1), 83–88. Hood, R.W., Jr. (1992). Sin and guilt in faith traditions: Issues for self-esteem. In J.F. Schumaker (Ed.), Religion and mental health (pp.110–121). New York: The Guilford Press. Hood, R.W., Jr., Spilka, B., Hunberger, B. & Gorsuch, R. (1996). The psychology of religion: An empirical approach (2nd ed.). New York: The Guilford Press. Hunter, J.A., Platow, M.J., Howard, M.L. & Stringer, M. (1996). Social identity and intergroup evaluative bias: Realistic categories and domain specific self-esteem in a conflict setting. European Journal of Social Psychology, 26(4), 631–647. Hunter, J.A., Stringer, M. & Watson, R.P. (1991). Intergroup violence and intergroup attributions. British Journal of Social Psychology, 30, 261–266.
Idler, E.L. (1995). Religion, health and non-physical senses of self. Social Forces, 74(2), 683–704. Jacobson, J. (1997). Religion and ethnicity: Dual and alternative sources of identity among young British Pakistanis. Ethnic and Racial Studies, 20, 238–250. Jacoby, M. (1997). Shame and the origins of self-esteem: A Jungian approach. London: Routledge. King, V., Elder, G.H. & Whitbeck, L.B. (1997). Religious involvement among rural youth: An ecological and lifecourse perspective. Journal of Research on Adolescence, 7(4), 431–456. Kirkpatrick, L.A. (1998). God as a substitute attachment figure: A longitudinal study of adult attachment style and religious change in college students. Personality and Social Psychology Bulletin, 24(9), 961–973. Koenig, H.G., George, L.K., Hays, J.C., Larson, D.B., Cohen, H.J. & Blazer, D.G. (1998). The relationship between religious activities and blood pressure in older adults. International Journal of Psychiatry in Medicine, 28(2), 189–213. Koenig, H.G., Pargament, K.I. & Nielsen, J. (1998). Religious coping and health status in medically ill hospitalised older adults. Journal of Nervous and Mental Disease, 186(9), Kolchakian, M.R. & Sears, M.F. (1999). Religious coping in college students. Journal of Religion and Mental Health, 38(2), 115–125. Kubacka-Jasiecka, D., Dorcazk, R. & Opoczynska, M. (1996). The role of religious values in functioning and mental health. In H. GrzymalaMoszczynska & B. Beit-Hallahmis (Eds.), Religion, psychopathology, and coping (pp.235–243).
Lawson, M. (1997). Struggles for mutual reverence: Social Strategies and religious stories. In Contemporary American religion: An ethnographic reader (pp.51–58). Walnut Creek, CA.: Alta Mira Press. Lea, G. (1982). Religion, mental health and clinical issues. Journal of Religion and Health, 21, 336–351. Levin, J.S. & Markides, K.S. (1986). Religious attendance and subjective health. Journal for the Scientific Study of Religion, 25(1), 31–40. Levin, J.S. & Vanderpool, H.Y. (1987). Is frequent religious attendance really conducive to better health?: Towards an epidemiology of religion. Social Science and Medicine, 24(7), 589–600. Levin, J.S., Wickramasekera, I.E. & Hirshberg, C. (1998). Is religiousness a correlate of absorption? Implications for psychophysiology, coping and morbidity. Alternative Therapies in Health and Medicine, 4(6), 72–76. Lewis, C.A. (1999). Is the relationship between religion and personality ‘contaminated’ by social desireability as assessed by the Lie Scale?: A methodological reply to Eysenk (1998). Mental Health, Religion and Culture. Lewis, H.B. (1971). Shame and guilt in neurosis. New York: International Universities Press. Liao, K.L.M., Hunter, M. & Weinman, J. (1996). Health-related behaviours and their correlates in a general population sample of 45-year-old women. Psychology and Health, 10(3), 171–184. Loewenthal, K.M. (1995). Mental health and religion. London: Chapman & Hall. Loewenthal, K.M. (2000). The psychology of religion: A short introduction. Oxford: Oneworld.
Loewenthal, K.M. & Cinnirella, M. (1999). Beliefs about the efficacy of religious, medical and psychotherapeutic interventions for depression and schizophrenia from different cultural-religious groups in Great Britain. Transcultural Psychiatry, 36(4), 491–504. Loewenthal, K.M., Cinnirella, M., Evdoka, G. & Murphy, P. (2001). Faith conquers all? Beliefs about the role of religious factors in coping with depression among different cultural-religious groups in the UK. British Journal of Medical Psychology, 74(3), 293–303. Loewenthal, K.M., Goldblatt, V., Lubitsch, G., Gorton, T., Bicknell, H., Fellowes, D. & Sowden, A. (1997). The social circumstances of anxiety and its symptoms among Anglo-Jews. Journal of Affective Disorders, 46, 84–97. Luyten, P., Corveleyn, J. & Fontaine, J.R.J. (1998). The relationship between religiosity and mental health: Distinguishing between shame and guilt. Mental Health, Religion & Culture, 1(2), 165–184. Makins, M., Adams, D. & Knight, L. (Eds.). (1997). Collins shorter dictionary and thesaurus. Glasgow: Harper Collins Publishers. Maltby, J., Macaskill, A. & Day, L. (2001). Failure to forgive self and others: A replication and extension of the relationship between forgiveness, personality, social desirability, and general health. Personality and Individual Differences, 30, 881–885. Markstrom, C.A. (1999). Religious involvement and adolescent psychosocial development. Journal of Adolescence, 22(2), 205–221. Markstrom, C.A., Berman, R.C. & Brusch, G. (1998). An exploratory examination of identity formation
among Jewish adolescents according to context. Journal of Adolescence Research, 13(2), 202–222. Maton, K.I. (1989). The stress-buffering role of spiritual support: Crosssectional and prospective investigations. Journal for the Scientific Study of Religion, 28(3), 310-–323. Mauger, P.A., Perry, J.E., Freeman, T., Grove, D.C., McBride, A.G. & McKinney, K.E. (1992). The measurement of forgiveness: Preliminary research. Journal of Psychology and Christianity, 11, 170–180. McCullough, M.E. & Worthington, E.L., Jr. (1995). Promoting forgiveness: A comparison of two brief psychoeducational group interventions with a waiting list control. Counselling and Values, 40, 55–68. McCullough, M.E., Worthington, E.L. & Rachal, K.C. (1997). Interpersonal forgiving in close relationships. Journal of Personality and Social Psychology, 73, 321–336. McKinney, J.P. & McKinney, K.G. (1999). Prayer in the lives of late adolescents. Journal of Adolescence, 22(2), 270–290. Meek, K.R., Albright, J.S. & McMinn, M.R. (1995). Religious orientation, guilt, confession and forgiveness. Journal of Psychology and Theology, 23, Melia, S.P. (1999). Continuity in the lives of elder Catholic women religious. International Journal of Ageing and Human Development, 48(3), 175–189. NHS Centre for Reviews & Dissemination (1996). Undertaking Systematic Reviews of Research on Effectiveness (March). York: University of York. O’Connor, K.V. (1983). The structure of religion: A repertory grid approach.
Unpublished doctoral thesis, University of New South Wales, Australia. O’Connor, K.V. (1998). Religion and mental health: A review of Antoine Vergote’s approach on guilt and desire. International Journal for the Psychology of Religion, 8(2), 125–148. Paloma, M.M. & Gallup, G.H. (1991). Varieties of prayer. PA: Trinity Press. Pargament, K.I. (1997). The psychology of religion and coping: Theory, research practice. New York: The Guilford Press. Pargament, K.I. & Rye, M.S. (1998). Forgiveness as a method of religious coping. In E.L. Worthington Jr. (Ed.), Dimensions of forgiveness: Psychological research and theological perspectives (pp.59–78). London: Templeton Foundation Press. Payne, I.R., Bergin, A.E., Bielema, K.A. & Jenkins, P.H. (1991). Review of religion and mental health: Prevention and the enchantment of psychosocial function. Prevention in Human Services, 9, 11–40. Payne, I.R., Bergin, A.E., Bielema, K.A. & Jenkins, P.H. (1992). Review of religion and mental health: Prevention and the enhancement of psychosocial functioning. In K.I. Pargament, K.I. Maton & R.E. Hess (Eds.), Religion and prevention in mental health, research, vision, and action (pp.57–82). New York: The Haworth Press. Pettigrew, T. (1979). The ultimate attribution error: Extending Allport’s cognitive analysis of prejudice. Personality and Social Psychology Bulletin, 5, 461-476. Pruyser, P.W. (1987). Where do we go from here? Scenarios for the psychology of religion. Journal for the Scientific Study of Religion, 26(2),
Ressler, W.H. (1997). Jewishness and well-being: Specific identification and general psychological adjustment. Psychological Reports, 81(2), Richards, P.S. (1991). Religious devoutness in college students: Relations with emotional adjustment and psychological separation from parents. Journal of Counselling Psychology, 38(2), 189–196. Rokeach, M. (1960). The open and closed mind. New York: Basic Books. Rosenberg, S. & Gara, M.A. (1985). The multiplicity of personal identity. In P. Shaver (Ed.), Review of personality and social psychology (Vol. 6) (pp.87–113). Thousand Oaks, CA: Sage Publication. St. George, A. & McNamara, P.H. (1984). Religion, race and psychological well-being. Journal for the Scientific Study of Religion, 23, Sanua, V.D. (1969). Religion, mental health and personality: A review of empirical studies. American Journal of Psychiatry, 125, 1203–1213. Schumaker, J.F. (1992). Mental health consequences of irreligion. In J.F. Schumaker (Ed.), Religion and mental health (pp.54–69). New York: Oxford University Press. Silverman, G. & Oglesby, W.B. (1983). The new birth phenomenon during imprisonment: Corrective emotional experience or flight into health? Pastoral Psychology, 31(3), 179–183. Stark, R. (1971). Psychopathology and religious commitment. Review of Religious Research, 12, 165–176. Tajfel, H. (1978). Differentiation between social groups. London: Academic Press. Tajfel, H. & Turner, J. (1986). The social identity theory of intergroup behaviour. In S. Worchel &
W.G. Austin (Eds.), Psychology of intergroup relations. Chicago: Nelson. Tangney, J.P. (1995). Shame and guilt in interpersonal relationships. In J.P. Tangney & K.W. Fischer (Eds.), Selfconscious emotions: The psychology of shame, guilt, embarrassment and pride (pp.114–139). New York: The Guilford Press. Tangney, J.P. (1996). Conceptual and methodological issues in the assessment of shame and guilt. Behavioural Research and Therapy, 34(9), 741–754. Tangney, J.P., Burggraf, S.A. & Wagner, P.E. (1995). Shame-proneness, guiltproneness, and psychological symptoms. In J.P. Tangney, & K.W. Fischer (Eds.), Self-conscious emotions: The psychology of shame, guilt, embarrassment and pride (pp.343–367). New York: The Guilford Press. Tangney, J.P., Wagner, P. & Gramzow, R. (1992). The test of self-conscious affect. Fairfax, VA: George Mason University. Tate, E.D. & Miller, G.R. (1971). Differences in value systems of persons with varying religious orientations. Journal for the Scientific Study of Religion, 10(4), 357-365. Toulmin, S.E. (1958). The uses of argument. Cambridge, UK: Cambridge University Press. Treffry, D. & Ferguson, S. (2002). Collins Paperback Dictionary. Glasgow: Harper Collins Publishers. Van Uden, M.F.H. & Pierper, J.Z.T. (1996). Mental health and religion: A theoretical survey. In H. GrzymalaMoszczynska & B. Beit-Hallahmi (Eds.), Religion, psychopathology and coping (pp.35–55). Amsterdam: Rodopi. Ventis, W.L. (1995). The relationships between religion and mental health. Journal of Social Issues, 51(2), 33–48.
Vergote, A. (1988). Guilt and desire: Religious attitudes and their pathological derivatives. New Haven: Yale University Press. Verter, B.J. (1998). Spiritual capital: Why Madonna studies Kabbalah. Unpublished paper presented at Franklin and Marshall College. Vingerhoets, A.J., Croon, M., Jeninga, A.J. & Menges, L.J. (1990). Personality and health habits. Psychology and Health, 4(4), 333–342. Watson, P.J., Morris, R.J. & Hood, R.W. (1987). Anti-religious humanistic values, guilt and self-esteem. Journal for the Scientific Study of Religion, 26(4), 535–546. Watson, P.J., Morris, R.J., Hood, R.W., Milliron, J.T. & Stutz, N.L. (1998). Religious orientation, identity and the quest for meaning in ethics within an ideological surround. International Journal for the Psychology of Religion, 8(3), 149–164. Worthington, E.L. (Ed.). (1998). Dimensions of forgiveness: Psychological research and theological perspectives. PA: Templeton Foundation Press.
Wulff, D.M. (1997). Psychology of religion: Classic and contemporary (2nd ed.). New York: John Wiley & Sons, Inc. Wuthnow, R. (2000). How religious groups promote forgiving: A national study. Journal for the Scientific Study of Religion, 39(2), 125–139. Zinnbauer, B.J., Pargament, K.I., Cole, B., Rye, M.S., Butter, E.M., Belavich, T.G., Hipp, K.M., Scott, A.B. & Kadar, J.L. (1997). Religion and spirituality: Unfuzzying the fuzzy. Journal for the Scientific Study of Religion, 36(4), 549–564.